Recently the California Legislative Analyst’s Office (LAO) released a report on special education in California, Overview of Special Education in California. The report goes over many details of special education, but I will focus on only a few here.
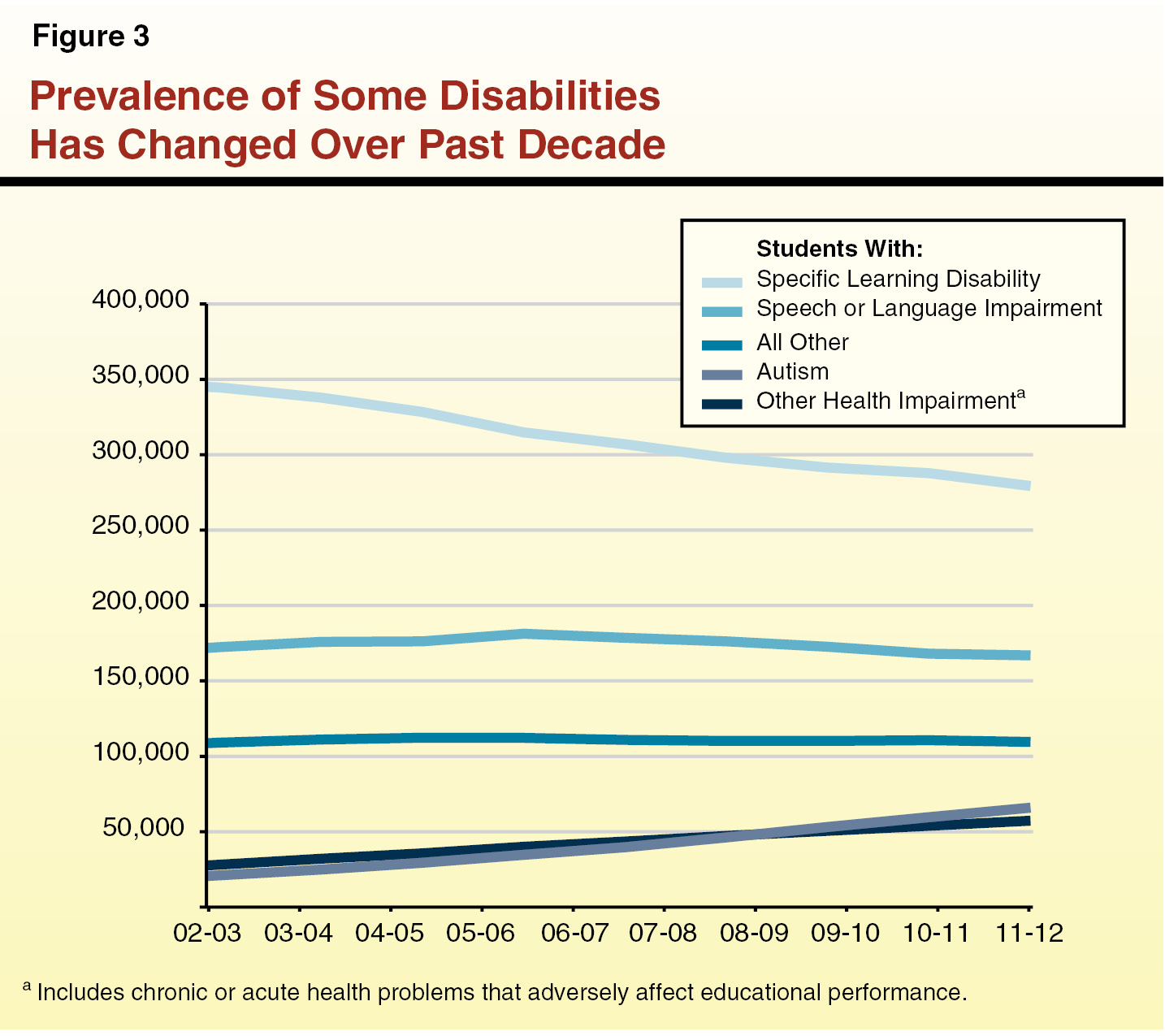
First, the time trend. Yes, the number of students receiving services under the autism label is going up.

Then again, no sign that it is going down after the removal of thimerosal. Also worth noting is the fact that other health impairments as a category is also increasing. Specific Learning Disability is going down. So it’s a bit more complex than just “autism is going up”.
What interests me more is the discussion of costs and finances. On term that often bothers me is the term “encroachment”. As in, “special ed students cost more, and that is an encroachment on the funds for the regular education students”. The LAO report discusses one aspect of that misconception:
(Note: SWD are “students with disabilities”)
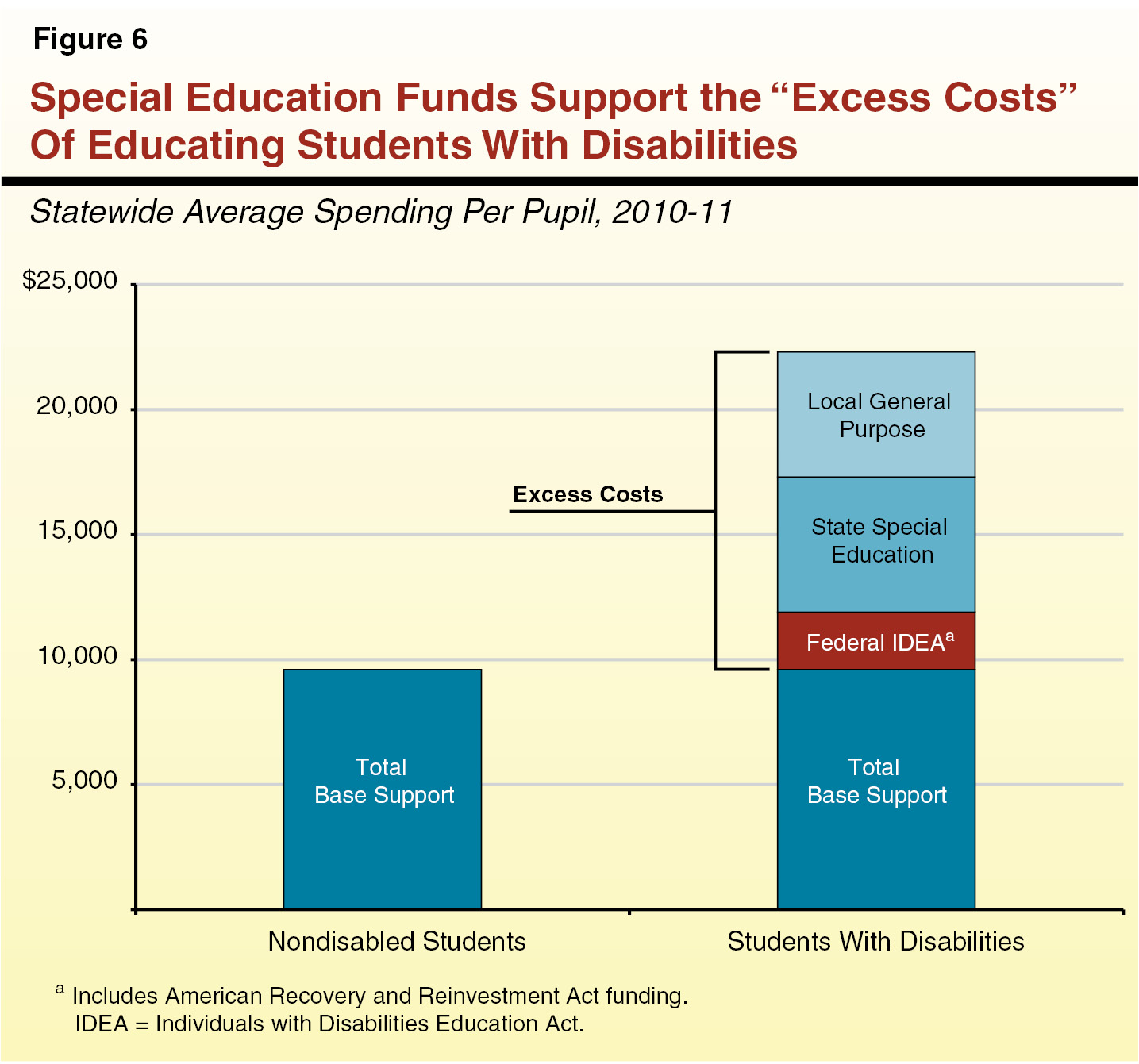
Misconceptions About “Encroachment” Some local educational agencies (LEAs) complain that local contributions for special education “encroach” upon their general education programs, sometimes implying that any local dollar spent towards educating a student with disabilities (SWD) imposes unfair expenditure requirements on their general purpose budgets. This argument, however, is a mischaracterization of both federal and state laws. Federal Individuals with Disabilities Education Act (IDEA) and state special education categorical funds never were intended to cover the full costs of educating a SWD—instead the bulk of the “regular” education costs are intended to be covered using local revenue limit and categorical funding, just as for nondisabled students. Moreover, federal IDEA and state special education categorical funds never were intended to fully cover the excess costs of educating a SWD—the special education funding model always has been predicated on a three–way cost–sharing model, including local sources. Despite this basic design of the funding model, LEAs sometimes express frustration that their local share of special education costs is too high. This frustration tends to increase as their local share of special education costs increases, as this leaves them with fewer resources to serve other students.

Schools are required to provide free appropriate public education (FAPE) to all students, not just students with disabilities. Some students cost more, some cost less, some cost much more. In California, on average, schools spend $9,600 per non disabled student and, on average, $22,300 per disabled student. Where does that money come from to pay for the disabled student’s costs? Well, $9,600 comes from the money the school would spend anyway. The rest is: $2,300 in federal funds, about $5,400 in state funds, and about $5,000 local funds. So, the “extra” cost for special education students is largely paid by state and federal funds. The Federal government has never paid the full amount they committed for special education. The LAO notes:

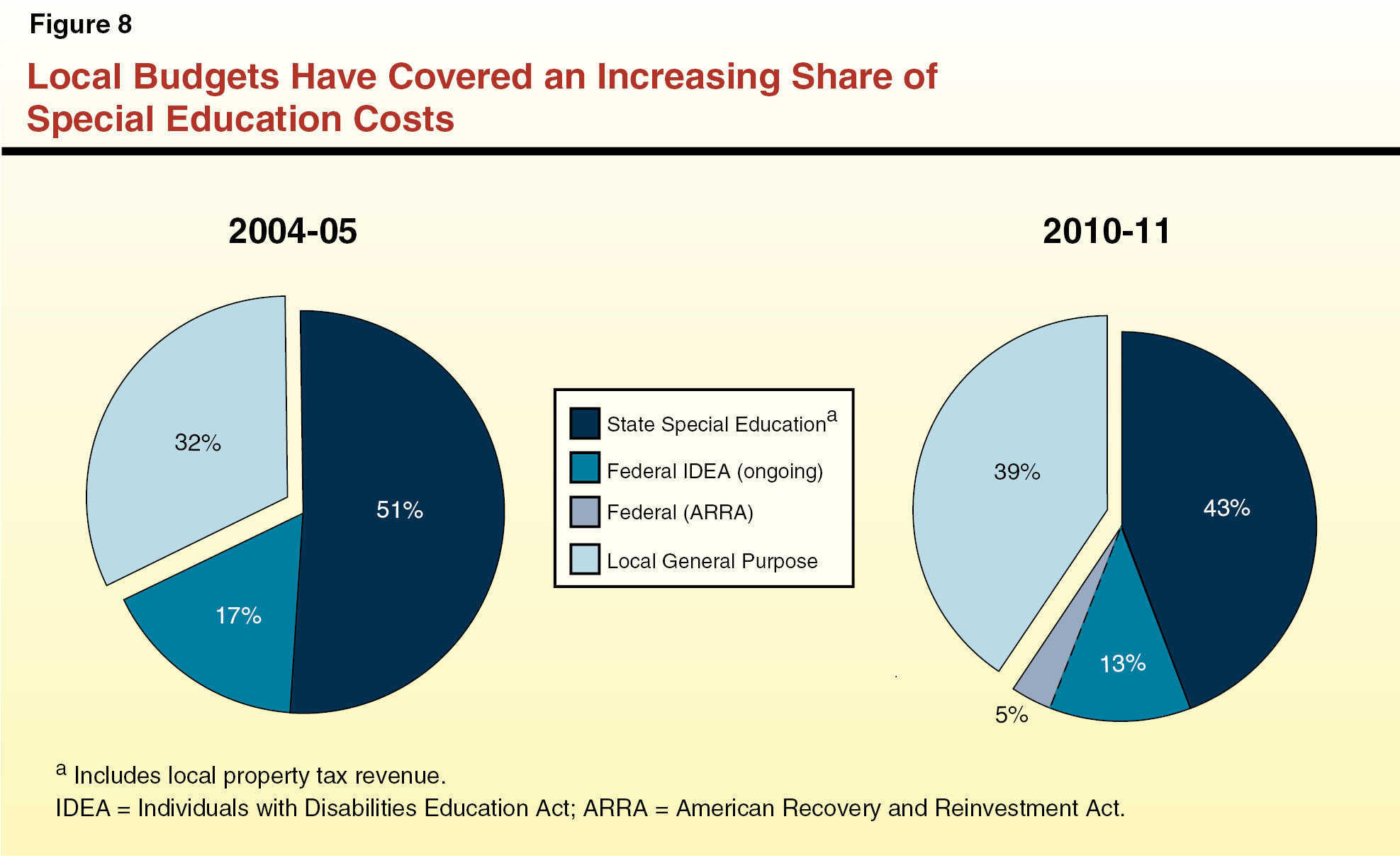
Federal Share Has Never Reached Intended Contribution Level. As shown in Figure 8, federal IDEA funds typically cover less than 20 percent of overall special education expenditures. This is notably lower than the amount the federal government originally committed to provide in support of special education services. The IDEA expresses intent to appropriate funding for each SWD up to 40 percent of the national average expenditure level per K–12 pupil, which would equate to roughly 40 percent of California’s overall special education expenditures. The federal budget, however, has never come close to providing states with this amount. We estimate that California would receive roughly $2 billion more annually if the federal government were to “fully fund” the intended level articulated in the IDEA.
If the Federal Government made good on it’s promise, it would be a great help to education. How’s that for an obvious statement. Somehow this obvious fact hasn’t made an impression on our legislators. That all said–just because the Federal Government isn’t helping as much as they should, that doesn’t mean that cost is an “encroachment” by special ed students.
Now, how does the state decide how much to give to each school district? It isn’t based on “your expenses are $XX, so we will give you a fraction of that.” It isn’t based on, “You have so many special ed students, so we will give you $YY per special ed student.” No, it’s, “your student population is ZZZ, so we give you money based on that number.”
In other words, if a school district has 100% special students, they get the same funding as if they have 0%. If the costs are high or low, they get the same amount from the State and Federal Governments. This isn’t the full story, but it is close:
Two Distribution Models Exist. Across the nation, states generally use one of two approaches to distribute special education funding to the local level. Some use a “cost–based” model, with funding allocations driven by how many SWDs are served or the magnitude of special education costs incurred. In contrast, other states rely primarily on a census–based funding methodology that is not linked to particular SWDs. Under this model, the state allocates special education funds based on the total number of students enrolled, regardless of students’ disability status. This funding model implicitly assumes that SWDs—and associated special education costs—are relatively equally distributed among the general student population and across the state. While the majority of federal special education funds are distributed using a census–based model, the IDEA formula does allocate a small portion (typically around 10 percent) of funds based on counts of economically disadvantaged students, on the assumption that this group contains a greater proportion of SWDs.
A district (or SELPA or LEA) gets paid the same amount whether a student is receiving services for special education or not. Whether a student’s special education services cost a little or a lot. And some districts feel that some or all dollars spent on special education are “encroachment”. We can complain, but in the end we’ve built a system which strongly disincentivises schools from taking a true “cost blind” approach to finding an appropriate education.
—
By Matt Carey



Recent Comments