
If you’ve been reading about autism online, you have almost certainly read that autism “rates” are on the rise. But what if I told you that here in California intellectual disability has been dropping for over 20 years?
For many years the mainstay of the “autism is an epidemic” idea was the California Department of Developmental Services data. The CDDS keeps track of how many Californians are getting support under a number of specific disability categories. These data are publicly available (although not as easily available in the past), which makes them an easy source of data.
It’s easy to take a cursory look at the CDDS data and think “these are official data. Look at how much autism has increased!” Or claim “the CDDS only serves “severe” autism, there’s no way they were missed in the past.” You can even find a few publications to cite to back up these observations.
About a year ago I asked CDDS for some data. I hadn’t checked in a while and I wanted to see what trends are ongoing. Coincidentally, the Autism Society of San Francisco put out a report shortly after that: Autism Rising, A Report on the Increasing Autism Rates in California. So I was not alone in asking for data. The Autism Society of San Francisco made the argument that the CDDS data are accurate and show an epidemic.
The Autism Society of San Francisco graph the data in many different ways, but the one that was closest to the way I was looking at the data was in Figure 5 (click to enlarge):
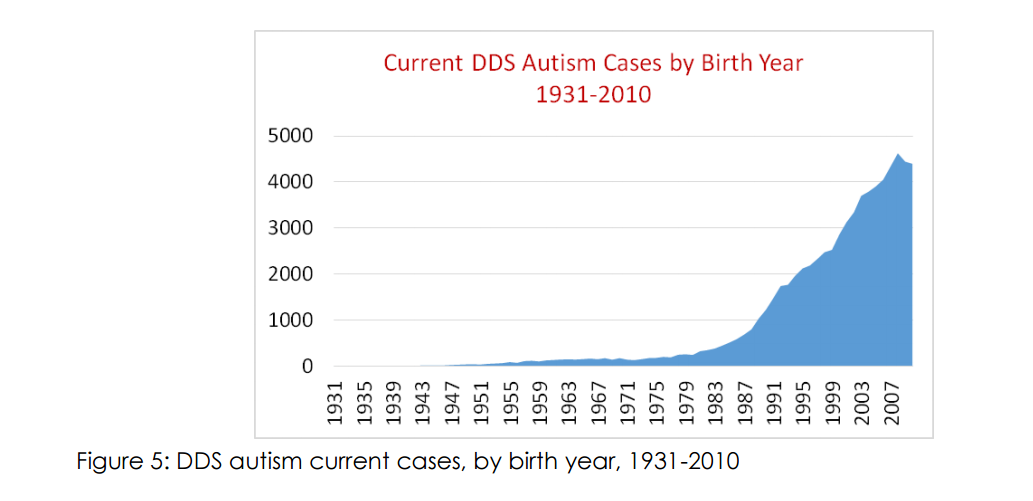
and here is the caption for Figure 5:
Births of individuals later deemed to have DDS-eligible autism have been increasing sharply every year since the early 1980s. Typically intake into the system occurs between 2 and 7 years of age. The data reflects about 200 DDS autism births per year into the 1980s, but now the system is reflecting nearly 5,000 such births per year. The drop off in cases after birth year 2008 is likely attributable to usual delay in cases entering the system, and likely does not represent an actual decrease in DDS-eligible autism cases.
You can stop there and support your argument. And that’s just what most people do. Or you can question–how can I test if this is a “real” autism increase? For example, is the autism rate the same among different races? The answer is no. Is the autism rate the same in, say, San Francisco, Los Angeles, and Kern County? The answer is no. And there are many more questions one can ask of these data and over and over, the answer is no.
Either we aren’t counting all the autistics in our state, or there is something much more complex going on than vaccine, toxins, epigenetics, or whatever the claimed causes of the rise are. And I’ve gone through many of these discussions over the years. Let’s make this simple then. If one claims that the CDDS counts everyone within each disability category accurately and that the definitions they use aren’t changing with time, why is intellectual disability (mental retardation) dropping so fast in California?
You see I also graphed intellectual disability. I got autism counts, intellectual disability counts and “unduplicated” (total, each disabled person counted once) by birth year. I also got census data by birth year. And I graphed them. And anyone claiming CDDS data show an autism epidemic needs to do the same and to explain this graph, complete with the sharp peak for birth year 1993. (click to enlarge):
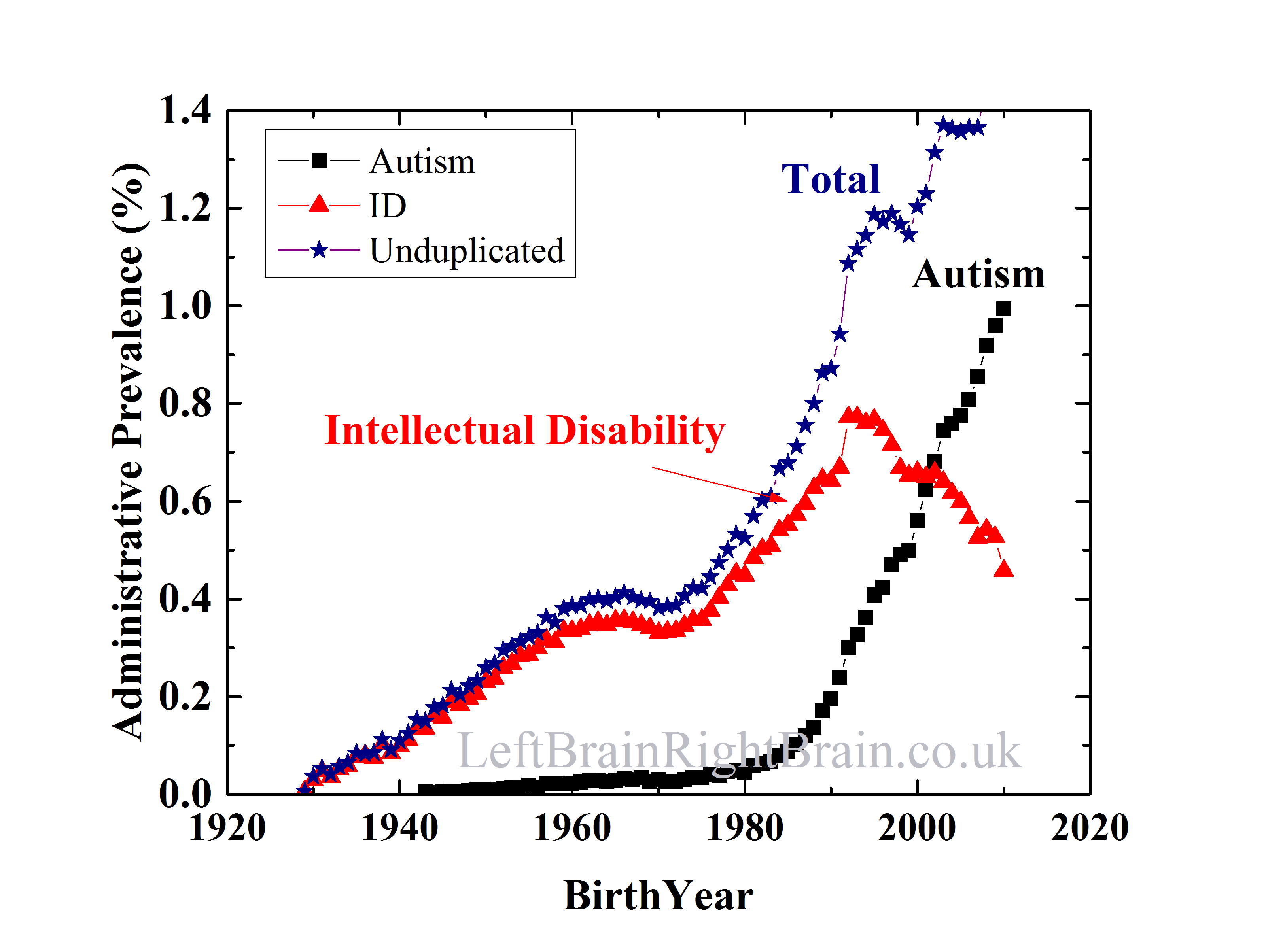
Intellectual disability has dropped. Off about 40% of the peak value.
If you think your idea for the rise in autism is correct, let’s take the failed vaccine idea as an example, you need to also explain how that resulted in far fewer people with intellectual disability. Plain and simple. And none of these claimed causes of an “epidemic” can explain the drop in ID.
Why bother challenging the people claiming an autism epidemic? Because it denies the existence of undiagnosed autistic adults. We have very little effort to identify those who were missed in past generations. And the likelihood is that these people–our people–are not being supported appropriately because of their misdiagnoses. And not only are we abandoning the misdiagnosed, we are failing to learn. What worked for past generations, the adults of today? What failed? What are the appropriate supports for the various needs of autistic adults? We don’t know today. And are unlikely to know by the time my kid is an adult, especially if we aren’t even looking at autistic adult needs today.
And then there’s the whole autism causation question. People spending their time trying to correlate CDDS data–data clearly confounded by numerous social influences–are unlikely to ever find a real answer.
But, for those who want to keep trying, include all the data. Give an explanation for this and you may be on to something.
—
By Matt Carey

Great article Matt.
Quite a bit less detailed than your analysis, but the national IDEA data collected yearly shows the same trends:
See Table 204.30.– Children 3 to 21 years old served under Individuals with Disabilities Education Act (IDEA), Part B, by type of disability: Selected years, 1976-77 through 2012-13, here:
http://nces.ed.gov/programs/digest/d14/tables/dt14_204.30.asp
Under “Percentage distribution of children served,” note the decreasing percentages in the disability categories of Intellectual Disability, Specific Learning Disability, Speech Language Impaired, and Emotional Disturbance as the percentage in the Autism category increases.
All while the “number served as a percent of total enrollment” (number of school children ages 3-21 served by IDEA via special education) – has actually been dropping for years (see 3rd table same link).
One might also note that Seneff has been relying on a completely brain-dead approach to IDEA data for years.
Excellent post!
Classic autism and aspergers are now autism which has made the spectrum even larger so now there are more diagnosed with autism Many with aspergers in the past were called just quirky. In the past many with juvenile autism were called retarded. There are more aspergers than there are autism with ID. Also many children with all types of ID are now called autistic. If you don’t know what’s I’m store for are children when they become adults than take a look around you. No more school, people are not lining up to hire them even though they are good at so many things. Many will still need services such as job coaches and continuing education and bus services. These young adults need something to do or the pacing will go on for the rest of their lives. That’s how important this issue is
Reblogged this on Eirene Hogan and commented:
This is an excellent post about the so-called ‘autism epidemic’ and how the increase in autism numbers is probably due to an equivalent decrease in the numbers of intellectually disabled (ID), ie, those formerly diagnosed as ID are now diagnosed as autistic. As the understanding of these conditions increases then the various conditions which cause an ‘intellectual disability’ is being teased out, hence the ID diagnosis will decrease but the other conditions will increase. In reality it is still the same number of people, they are just put into different criteria.
MR/ID is defined as having an IQ less than 70. These tests are standardized and the less able 2.2% of the population score less than 70. The number of people with MR/ID is therefore a constant percentage, but you can safely say it is less than 3% of a fairly large sample.
Clearly many people with ID have now been given the autism label.
At the other end, very intelligent, slightly quirky, people are now declaring themselves as “autistic”, but this is a dramatically different condition to what was called autism in previous years.
Saying “Oh but didn’t you know its a spectrum” is like a person with contact lenses comparing himself to a blind person because “we’re both just visually impaired”.
Much better to use the term Asperger’s and not drive the carers of people with Classic Autism completely crazy. They would fully support a campaign for Asperger’s awareness; which might mean the Public has a fighting chance of understanding what it is campaigners want them to be aware of.
Unfortunately many with autism have speech and language problems, and the IQ tests are very often language based. This is why my son was often given a low IQ, yet his more recent scores not as low as 70. He is literate, and is within a less then one standard deviation below the mean.
My son would have never been given an Asperger’s diagnosis because he was totally non-verbal when he was three years. One part of DSM IV is that only children who could speak were considered functioning enough to be Aspergers.
I am in no rush to measure my son’s IQ, but in most cases measured IQ in classic autism goes down as the person gets older, which upsets the parents. In typical kids they get cleverer as they get older and IQ tests take age into account. In classic autism cognitive dysfunction like disturbed excitatory/inhibitory imbalance (reversible with bumetanide) usually leads to a cognitive plateau in early childhood. Such kids usually “graduate” high school with academic skills of 4-7 year old.
Non-verbal IQ tests exist to test people who cannot speak.
People with Asperger’s do seem to have different biological variations to people who have speech delays and so it is good not to confuse them, particularly if you want to treat them.
“I am in no rush to measure my son’s IQ,…”
Unfortunately in our state it is kind of requirement to get Developmental Disabilities Administration services. These include respite hours, behavioral supports, some therapies and later supported employment and housing.
As those in the neurodiversity community like to remind us,autism is a spectrum.It isn’t all Asperger’s or high functioning autism on one end,and classic autism,and severe intellectual on the other.There are all kinds of shades of grey in between.My diagnosis was pretty much right in the middle of the spectrum.This meant I was verbal,with intact language,but very low functioning,in pretty much every other area,as well as having serious learning disabilities,though not classic ID.To use Peter’s description below mine,this meant completing high school with the academic skills of a 10 or 11 year old.As well as having many of the behavioural problems seen in low functioning autism.This might be considered “atypical” autism by some,but it is in keeping with autism seen with metabolic disorders,and other complex genetic diseases.I have multiple diagnoses in these areas.Anyone interested might want to take a look at this list.
Click to access 15.-Metabolic_Geneticist.pdf
Peter,
Yes, using the term autism for aspergers (which used to be called “The little Professors”) does for some reason tend to drive classic autism caregivers crazy. Why is that? Is it because regardless of the behavior s they have in common , there seems to be two different syndromes with different needs. And even someone said they have different brain structures.
There are definite biological similarities between severe autism and Asperger’s, but there are profound differences on a practical level. Asperger’s people can advocate for themselves and tell the world that they are happy how they are and do not want a “cure”, but some have extreme anxiety and there is a high suicide rate.
People with severe autism tend to die young, but not from suicide. They die early from seizures and accidents like drowning. People with severe autism cannot exist without their caregivers, who not surprisingly would give anything for a “cure”. When they hear people with mild/trivial “autism” say that the idea of a cure is “disgusting” they do go crazy; they find clearing up smeared feces disgusting.
So to anyone who does not have Asperger’s, it is pretty clear why the two groups do not get on. By definition, people with Asperger’s do not see the the other side of an argument. So no point to argue with someone with Asperger’s, they cannot change their view. This is probably not a good blog to point this out on.
There are 700+ autism genes, and so not surprisingly there are numerous sub-types of autism and Asperger’s.
My idea is call Asperger’s by that name and call autism by its name. Then everyone can be happy.
“Asperger’s people can advocate for themselves…”
Autistics can advocate for themselves as well. But they need help to make their advocacy be heard.
There are certainly times when my kid is advocating for a change. My kid may not understand the cure debate, so that’s not a part of the advocacy. We need to start making the world accept our children’s “voices” and real. Or, if we don’t accept that our kids are advocating, we can’t expect the rest of the world to do so.
“People with severe autism tend to die young, but not from suicide.”
Really? As one person recently discussed on this site, wandering/elopement may be a form of suicide for some.
Are you trying to provoke people with statements about “trivial” autism?
You may want to read Richard Grinker’s NYT editorial where he points out that the term “Asperger syndrome” does not mean mild. He gives the example of a classmate of his daughter’s who was diagnosed with AS. Said classmate had much greater autism-related challenges than his daughter (who is diagnosed with autistic disorder).
“My idea is call Asperger’s by that name and call autism by its name. Then everyone can be happy.”
It’s not a new idea. There are many reasons why the DSM 5 went exactly the opposite direction. The main reason is that researchers know it’s false. You may also want to consider how “everyone will be happy” when the evidence base for behavior therapies is based upon “high functioning” autistics. So your definition would leave those with “autism” without access to those therapies.
“By definition, people with Asperger’s do not see the the other side of an argument. So no point to argue with someone with Asperger’s, they cannot change their view. This is probably not a good blog to point this out on.”
True, this is a poor place to argue false ideas. Show me the definition of Asperger syndrome and tell me where this means they can not see the other side of an argument. You can not, because it is not in the definition of Asperger syndrome.
“When they hear people with mild/trivial “autism” say that the idea of a cure is “disgusting” they do go crazy; they find clearing up smeared feces disgusting.”
Given your approach to the discussion, one wonders how often you’ve insulted people by calling their disability “trivial”, but interpreted their response as being a result of other parts of your message. Thing is you probably don’t even see why you are the problem, you are the one derailing conversations.
My idea is call Asperger’s by that name and call autism by its name. Then everyone can be happy.
Not quite, how about using the same learning strategies used by aspies for autistics?
For this, I can only speak for myself but back in 1983, I was diagnosed with language development delay (I have the complete 600+ pages medical files of that time) and encephalopathy. In 2004, this was revised to autism by a medical scientist studying autism human subjects.
IQ:
1983: 80
2004: (research subject for a full battery of test), 113 and 119.
Remember, my diagnostic is autism as opposed to asperger. Could it be the same case for other autistics (and yes, I wanted to check out the epidemiological data regarding static level or declining level of IQ in autistics patients).
IMO, the diagnostic label is less important but does having the proper diagnostic allow for a good learning / life skill adaptation plan? _This_ _is_ what I have been thinking all along. Are we gonna put a set of blinder on the learning skill on aspies (and auties like me) or are we gonna use it to adapt the learning curve of autistic with ID?
Alain
Alain said, “Not quite, how about using the same learning strategies used by aspies for autistics?”
My son is autistic with a low IQ, he would have been diagnosed as ID in the old days. Trying to teach him the way you’d teach an aspie would get nowhere. Maybe they should try teaching them all in the way that suits them individually, instead of trying to find some blanket strategy.
eirenehogan: “Maybe they should try teaching them all in the way that suits them individually, instead of trying to find some blanket strategy.”
The first person in the school district to use the word “autism” for my son was the school psychologist his last year of high school when he was nineteen years old (he is now 27). She then told me that they had an “autism” program, but if he went into it he would lose services, which would not be useful.
Apparently while “if you met one autistic person, you have met juar one autistic person” was not really the mantra in that school. It seemed like if you have “a diagnosis of autism we’ll put you with others and bribe some other students to be peer examples” — even though you all have vastly different needs.
Eirene Hogan,
Ok, I get it that trying to teach an autistic the same way as an aspie would lead to nowhere with your child. Now, can we agree the devil’s in the detail and I was thinking about a similar general learning framework for both diagnoses which indeed, require adaptation to the individual.
All of this lead to a question: do you absolutely think that the teaching method should be totally different for autistics with ID, autistics without ID and aspies (requiring adaptation of course) or there can be similar ground in teaching methods? Totally different, or some similar aspect?
Alain
Peter, I think you have gone a little too far. I don’t like the terms LFA or HFA. So like it or not I will use the terms aspergers and classic autism. It is demeaning to think that all classic non verbal autisms are poop smearers with low IQ. I know this by going to different autism classrooms that maybe only one little boy did like to play in the toilet. Also people with aspergers are aware when they are being bullied. Not a good feeling. Try to show a little respect for humanity especially children who have challenges even beyond our understanding. When I think back (I am pretty old) in grade school one boy always got into trouble and the nuns used go make him sit in the waste basket. We never want go go back to when disabled children were sent to live in institutions. So love your child and do what you can even if he is little and head bumps you. That hurts!
Matt Carey said: “You may also want to consider how ‘everyone will be happy’ when the evidence base for behavior therapies is based upon ‘high functioning’ [autistic people].”
That’s incorrect, actually. Although the vast majority of autism research does tend to have autistic people perceived as ‘high functioning’ as participants, the vast majority of ABA research goes the other way in featuring people who may never speak a word and whose IQs are far from accurately measurable on the Wechsler Scales. See Lovaas 1987 to read about the type of autistic people he included in his studies. There’s not one person who might meet the criteria for Asperger’s syndrome or ‘high functioning autism’ amongst them.
There is a great deal incorrect there. Referring to some autistics as “slightly quirky” denies the challenges they face. Also, many seem to forget that in the early days autism diagnoses were not given to people with intellectual disability. So when we talk about what autism was called in previous years, it’s not what people today sometimes think of as “classic autism”.
the analogy you provide suggests that those with autism have zero abilities in certain areas (are blind).
Hello Matt,
I appreciate that you are more logical in your approach than many writers on this topic.
However, you imply a claim that there is no significant actual increase in autism prevalence in California based on the drop in the proportion with ID, while your graph clearly shows a huge increase in the total of autism + ID, not just a huge increase in the proportion with autism. Your data argue in favor of the conclusion that there is a very large increase in autism, after accounting for what may be a change in diagnostic preference for autism vs. ID, just not quite as large as the conclusion one would draw from looking only at CA-DDS autism prevalence.
Of course, neither version of the graphed prevalence data proves nor disproves whether there is a real increase in autism prevalence by birth year, which is what matters for epidemiology. There are other ways to do it…
You may well be right that none of the factors so far hypothesized to have caused an autism epidemic are logically consistent with explaining all of the changes in prevalence. That does not mean there isn’t an increase, nor than none of the hypothesized factors has any effect. Much of the work of explaining autism has yet to be done.
It does presume, in a sense, that there has *not* been a real decrease in intellectual disability; i.e., that the shift is all diagnostic, and has no basis in reality. For example, in the late 70s we started removing lead from paint and gasoline on the basis of adverse neurodevelopmental effects. One wonders what effect this action might have had on the number of people scoring < 70 on an IQ test? If removing lead from gasoline and paint had the effect of *increasing* IQ, what effect would that have on the ID line in the graph above?
Similarly, the Flynn effect seems to indicate gradually increasing IQ scores over time in industrialized countries, which again should have the effect of reducing the number of people < 70 IQ. How is this accounted for in this type of analysis?
One thing is for certain, the type of analysis we see here affords us no ability to introduce the possibility of two different things happening over the course of decades, the assumption is that because the graphs superimpose well, we cannot have simultaneously had less intellectual disability and more autism. I doubt it is that simple. That isn't to say that diagnostic substitution isn't a real phenomena, but rather, assigning a one to one equivalency seems to be largely be a matter of convenience.
Of course, the people using the information as evidence of an epidemic are guilty of more egregious binary processing with regard to interpreting this 'data'.
“However, you imply a claim that there is no significant actual increase in autism prevalence in California”
I do not. Perhaps you could tell me what particular part of the above article led you to this idea.
Hi Matt, that was my impression from the overall article, including the title. I wonder how others interpreted it?
If it’s not what you meant, would you please clarify what you did mean? Some possible examples include:
– There has been a significant actual increase in autism prevalence in California
or
– There isn’t enough information available (whether from DDS, various summaries or graphs of DDS data, or perhaps elsewhere) to be able to determine whether or not there is a significant real increase
– Etc.
The really interesting question is what is the true trend by birth year; that’s different from population prevalence.
In case you’re interested, my personal view is that this question has not been answered properly yet, and it’s difficult but not impossible to answer.
If you are using California data to claim an autism epidemic, you’re doing it wrong.
The data are so confounded by other influences (social in my opinion) that claiming that these data are a true prevalence is impossible. And if they aren’t a true prevalence, stating that the prevalence is going up, down or flat is impossible. Stating it isn’t going up, down or is flat is also impossible based on these data. A least in their raw form (which most people use).
As to the ID prevalence data: one either has to say “that’s ‘real’ too, and here’s how my model accounts for a big drop in ID”, or one has to say, “the ID data point strongly to some sort of social shift in the CDDS data, and I have to account for that before saying that there’s something really changing in autism prevalence.”
Two groups have used CDDS data to claim that older age of parents has led to an increase in the “real” prevalence. Interestingly, a recent study claims this isn’t due to some genetic mutations involved with older parents, but is instead due to the fact that people with more autistic traits tend to have kids later in life (I’m not convinced, but it’s an idea).
I once asked an epidemiologist if we would ever know exactly what the prevalence has been for the past, say, 30 years, and if we have a true increase. Said epidemiologist just looked back at me without answering.
A long while back I plotted CDDS datasets taken from different recent years. It was very interesting to see that autism prevalence for many years ago (say, 1980) went up. I’ll try to find the link. But that was a clear example that autism awareness and shifts in the understanding of what autism is was at play.
“However, you imply a claim that there is no significant actual increase in autism prevalence in California…”
He does not. Matt simply states the fact that there is no significant actual increase in autism prevalence in California. Can you grok the difference between the words ‘prevalence’ and ‘incidence’? I think not, I think not.
There are no new children being added to those receiving special education services in California.
This recent study presented at the Chapman University DisAbility Summit examines diagnostic migration from the category of Specific Learning Disability – there appears to be an anti-epidemic of SLD in CA as well:
WHY HAS THE RATE OF AUTISM INCREASED SO DRAMATICALLY? IT MAY NOT BE WHAT YOU THINK:
Click to access tpi-outcomes-summary-2016.pdf
• Contrary to media reports, the increase of autism is not adding kids to the number of children with disabilities.
• The increased rate of autism can be strongly explained by migration within disability categories. Diagnostic Migration.
• Environmental and human contributions do not account for an important increase in autism rates.
^Same study also discusses policy implications — including those for adults — as well as including this report (begins on page 12):
AUTISM IN THE WORKPLACE: A SPECIAL REPORT
Click to access tpi-outcomes-summary-2016.pdf
“• The increased rate of autism can be strongly explained by migration within disability categories. Diagnostic Migration.”
My son started in his special ed. preschool in 1991, when it was DSM III and there was no actual “autism” category under IDEA (okay, not in California, but still a west coast state). His particular preschool program was created in the late 1970s as a direct offshoot from the Hard of Hearing program because they were getting kids who could not speak but could hear.
These kids had a variety of “formal” diagnoses. My son was dyspraxic, but there was also Specific Learning Disability, childhood aphasia, childhood apraxia, hyperlexia and on and on.
As an aside: one year the dyspraxic preschool teacher went on sabbatical. There was a qualified substitute for one semester, but due to other conflicts, the kids in the “dyspraxic” program were combined with the dwindling Hard of Hearing program for the rest of the year (it worked out well, there were friendships made).
Being a typical mom, I kept so many things: including the class pictures with the names of the kids. So I google-stalked the names, and I got a few hits. One particular child who was a bubbly five year old twenty years before, is still a very bubbly adult with fairly severe autism (from a video promoting an adult autism day center), and then there were LinkedIn profiles of a couple of young men. One, who is doing very well, had graduated with a science degree, and the other did computer support (except his profile was a selfie while he was in his jammies, seems to be an autistic behavior, just by going by my son’s behavior).
Unfortunately there was some bad outcomes. One child had been jailed, and another had died.
This is only anecdata, but it does show why I am confident that the changes in diagnostic criteria is driving the “increase” in autism.
” (except his profile was a selfie while he was in his jammies, seems to be an autistic behavior, just by going by my son’s behavior).” Are sensory issues not part of the criteria for autism? Loud noises, fear of crowds, wearing clothes with tags, hair cuts etc., I thought were all part of autism. Severe ADHD, inability to concentrate, unable to sit still complicates things even more. These things have kind of faded away as he gets older. Is it because we took him places and became accustomed to his surroundings? It is good that the “dyspraxia” program worked out well. When I spoke of the past I did not mean to imply that kids in the past with Aspergers were quirky. It is just how we saw them from a classmate point of view back in the 50’s and 60’s. I was known as skinny and shy. Maybe today I would be diagnosed as anorexic with mute shyness. Never would I want to downplay the challenges faced by anyone. AUTISM IN THE WORKPLACE: A SPECIAL REPORT
Click to access tpi-outcomes-summary-2016.pdf
This was very helpful. Thank you. This website is very interesting.
“Are sensory issues not part of the criteria for autism? Loud noises, fear of crowds, wearing clothes with tags, hair cuts etc., I thought were all part of autism.”
Yes. But the inappropriate clothing is more part of not being in tune with social expectations, kind of part of not really understanding how other people think. As one psychologist told me it is part of an off kilter executive function.
Right now my son is going to a social/job coach. He is having to learn that he really needs to bathe and look presentable for a job. This is stuff we as parents have tried to teach him, but it seems that we are not who he wants to listen to. Which is all right, because we just want to be his parents and not his bosses.
We are just stumbling through. This is not something that was in any “What to Expect When You are Expecting” book. Twenty five years ago I even picked up their book on how to deal with toddlers/preschoolers and there was absolutely nothing on “What to Expect When Your Child Does Not Talk.”
“True, this is a poor place to argue false ideas. Show me the definition of Asperger syndrome and tell me where this means they can not see the other side of an argument. You can not, because it is not in the definition of Asperger syndrome.”
Not so much in the definition of Asperger’s,but certainly in the language used by many advocates of neurodiversity.Particularly those who speak about not wanting cures or treatments for autism.Many neurodiversity advocates do seem to speak in broad terms about autism,with their language,and offered solutions,skewed towards the higher functioning end of the spectrum.There is a belief among many,myself included,that such language means they are speaking for the entire spectrum as a whole,even if this is not their intention.
My problem with the definition of,and diagnostic criteria for autism,is that it does not go far enough.You can berate me all you want for saying this,but I think the diagnostic criteria (DSM ADOS,etc) for autism ought to be expanded to include a list of things like intellectual and learning disabilities,seizures,ataxias,self abusive behaviour,sensory difficulties,problems with motor coordination,delayed walking,etc.Even putting aside GI disease,and other medical disorders,there are too many neurodevelopmental,behavioural,and other brain related conditions associated with autism,that could,and should,be factored into the diagnosis and definition of autism.As well as the way autism is spoken about in the general discourse of society.One could even add comorbid mental illness that shows up in older children and adolescents with higher functioning autism.Suicide, related to mental illness,being a major cause of death in teens and adults with higher functioning autism.Not including these conditions,when speaking about autism,is whitewashing the condition.Making autism seem more benign,and less of a big deal than it is.
Thanks for that. The SLD numbers have been discussed online for many years (my guess is you were part of those discussions). Interesting to see that it was finally picked up by some researchers.
Great article! “Intellectual disability has dropped. Off about 40% of the peak value.”
How much has autism risen exactly since that peak value? Also exactly 40%? Or more than that?
Autism has risen by a bit more than ID has dropped. ID doesn’t account for the entire rise, but it’s likely a big piece. And any theory of why autism is rising needs to include this.
Thanks. What is the difference between the two? The decrease in ID and rise in autism? I’m just curious about how much can be explained by the drop in ID 🙂
One can’t explain the rise with the drop in ID. One could argue it’s plausible but without more data it can’t be called an explanation.
Which is pretty much the point of the above. Groups who use raw CDDS data to draw strong conclusions are fooling themselves and misleading others. Actual epidemiology can be done with these data but it’s not just a matter of asking for data, getting someone to graph it for you and calling it science or evidence.
And those who have done real epidemiology have found that large social influences are at play. For example, and this partially answers your question, Peter Headman’s group at Columbia found a large effect of diagnostic accretion. People who were labelled as only having ID in the past are often getting ID plus autism diagnoses today.
But people who call epidemic almost always ignore Bearman and his multiple studies.
They will often cite Hertz-Picciotto. They will say she could only account for about 25% of the rise in autism. They then–erroneously–claim that the rest of the rise is therefore “real”. (socially driven rises are real too, such as diagnostic accretion. But it’s a shorthand, even if it is inaccurate, to say “real”)
Bearman’s diagnostic accretion study showed that there were more forces at work than what Hertz-Picciotto explored. And there is nothing saying that there aren’t more forces at play.
For example. What is the effect of the huge media effort to raise awareness in the past decade? Literally hundreds of millions of dollars worth of advertising and this had no effect? They did it for no reason?
Now here is the real bottom line here: we are missing a lot of adults. It isn’t a question of whether there is a large population of undiagnosed autistic adults, it’s a question of how large the population is.
People who cling to the epidemic idea to the exclusion of the idea that adults are often undiagnosed and likely improperly served are failing. We need to be finding and serving these populations, not denying their existence.
Not only is this just the right and good thing to do, it serves the goals of advocating for the next generation of autistics better than crying epidemic.
Something is lost in the translation. Currently, just about everyone in the planet define autism as a cluster of symptoms while a few (myself included) goes beyond and look at the brain biology (MRI, minicolumns) and the last few peoples digging into this biological data even thought it’s not part of the criteria used in the DSM, the ADI-R or the ADOS. Furthermore, for the last two diagnostic criteria, there is a mandate that inter-raters score are within the 90th percentile on a set of subjects (autistic or not) to be certified as competent in the diagnostic process of autism.
Where does that leave us? Very simple, the autistic children and adult have an extremely similar brain architecture regardless of IQ or any life adaptation skills. That brain architecture is vastly different as compared to a neurotypical one. Now all of you pointing out that autistic having an IQ over 100 are vastly different as compared to the retarded one are, in my not so humble opinion, as scientifically driven as the average naturopath and do trust me, I get better services from human resources managers as compared to the local autism job finding organism which is fully staffed with psycho-educators and social workers.
Finally, to expand on my last point (psycho-ed, social workers), we don’t need educatorsplaining and a glass ceiling over our head because it impose coping strategies to develop ourselves to a better level that the glass ceiling allow for. Can we have a little autonomy and be able to dictate the kind of help we need when we exhausted all our capacities.
Peter, I’m looking at you specifically (Saying “Oh but didn’t you know its a spectrum” is like a person with contact lenses comparing himself to a blind person because “we’re both just visually impaired”.) Assess the current biological data and come back to me with the same statement.
Alain
“Now all of you pointing out that autistic having an IQ over 100 are vastly different as compared to the retarded one are, in my not so humble opinion, as scientifically driven as the average naturopath …”
I never said that. I just pointed out it is difficult to get an IQ from a nonverbal child, and there is great variation.
It would be great to have MRI data from many more brains, but that is not possible. My son has been asked to participate in a study that included blood draws and an MRI. When he got the consent forms he refused on the basis they wanted video him.
I would like to point out that the criteria for autism varies between the school district and the states’ disability services department. The California Department of Disability Services is not part of the educational department.
Plus the criteria for getting services under “autism” varies by state. I am presently going to a series of workshops trying to figure out the complexities of our state’s system. Apparently those who move from California are disappointed with our state provides, while those who move from Idaho are delighted because it is more than what they are used to. So another reason why state data can be not sufficient.
At one workshop on eligibility for disability services a parent of someone with Down Syndrome was not happy that the IQ component for eligibility was much higher for autism than other disabilities. Being confused I looked it up, and there it was:
https://www.dshs.wa.gov/dda/consumers-and-families/eligibility
If you scroll down to the second to last table you will see that while adaptive skills for autism need to be two standard deviations below the mean, the Full Scale IQ only needs to be only one standard deviation below the mean.
Then on the next box down for “Another Neurological or Other Condition Similar to Intellectual Disability” the Full Scale IQ needs to be 1.5 standards below the mean.
Long story short: no one in my state with autism gets disability services if they have an IQ anywhere near or above 100 (unless they meet all of the points under DSM IV).
Chris,
You do understand, my reply wasn’t directed at you but more pointing out that, at the very least, a whole host of professions around autism (exception made of medical doctors but in their case, they refer to specialist) don’t look beyond the science they produce and, regarding IQ, it’s not the end-all be-all because of that simple fact: IQ less than 70 up to IQ around 140 (myself, I’m at 119 on the raven and 113 on the WAIS-III), same brain architecture exception made of minor variation which we also see in neurotypical brains but, completely different ways of functioning because exactly of these biological findings.
Basically, to paraphrase Orac, medicine will never be a science but it has to be as scientifically driven as possible and I’m not seeing that in the associated autism professions which, may at certain point, include public policies. I’m not seeing that.
Best regards,
Alain
I agree that autism is biological. Brain structure even down to the genetic makeup
I think the psychologists who make up the rules can only look at behavior. I have read that those with autism have no empathy
and I don’t believe that. maybe they don’t know how to express it. Also that they don’t love and again they have to learn to show affection
IQ score can’t determine if you are good or happy or funny
Most of what you have wrtten I truly can’t comprehend so maybe you are way smarter than I am.
Just replied to Chris but my comment vanished, am I under moderation?
Alain
Probably just being quirky. Perhaps Matt will find it after work.
I’ll wait but just a quick word to say my previous comment wasn’t directed at you. I know you fully understand the crater between research and clinical practice and furthermore, public policies.
Alain
Okay dokay. I understand a bit since I am so close to some researchers, and am actively trying to get our family enrolled in the large genetic study. At least that one only uses spit. No blood draws nor MRIs required, just son has to be the to sign us up.
Roger is correct
There are shades of grey on the spectrum. We never had to deal with wandering off or poop smearing or huge meltdowns. He can’t talk but he looks things up on the computer such as how do airplanes fly or whats playing at the cinemas. He won’t get a cause or cure in his lifetime but I hope he continues to have a good quality of life. He doesn’t have any friends because he doesn’t know how but he hangs out at the peripheral listening with a smile. There is a person at school he calls Michael who is interested in the same things
but when they see each other outside of school, they don’t even say hi. As for IQ I don’t want to know because he is quick and smart in some ways and not in others. Not quite an “idiot savant” as they used to call them.
“As for IQ I don’t want to know because he is quick and smart in some ways and not in others. Not quite an “idiot savant” as they used to call them.”
That totally describes my adult son (who was diagnosed when he was 26 years old!)s Today his social coach found out he can actually cook and had memorized recipes. That is all good, but both dishes are time consuming and do not provide sufficient nutrition. The problem is expanding his food choices to things that are quick to make, nutritious and affordable with his food benefits.
To be truthful he poop smeared once (that was amusing), but his “terrible twos” lasted for about two weeks. For his younger brother I dealt the “terrible twos” from the time he was eighteen months until he was seven years, plus he only became potty trained just before entering kindergarten! (younger child turned out to be extremely normal, has a real job and is the trustee protector for his older brother’s special needs trust.
Thank you for posting this – as the key issue in your blog; which ironically this issue (this point) could become lost within the thread(s) that followed:
“”Now here is the real bottom line here: we are missing a lot of adults. It isn’t a question of whether there is a large population of undiagnosed autistic adults, it’s a question of how large the population is.
People who cling to the epidemic idea to the exclusion of the idea that adults are often undiagnosed and likely improperly served are failing. We need to be finding and serving these populations, not denying their existence.
Not only is this just the right and good thing to do, it serves the goals of advocating for the next generation of autistics better than crying epidemic.”
As you highlight – rising graph lines here- declining graph lines there…yes, it is time to take a deep breath and unpack the data vs. the interpretation that follows (make that: interpretations – plural). While the data can scream out “epidemic” or “tsunami” – this has a double-edge effect of leading to a child-centric perspective of autism- and create a demographic bias of losing sight or interest or effort – to address the lifelong conditions of autism. From a gerontological perspective – “aging out” is in effect – “aging in” – back into the life course for the long haul of adulthood and aging. If you would look at the piechart for actual and % dollars in autism research – and then compare the “slices” – you will see that the focus on life course (life span – assuming this means beyond transition years) is but a sliver (1%) compared to other funding “priorities.”
Have you addressed this response to your piece yet? http://www.sfautismsociety.org/blog/setting-the-record-straight-about-the-alarming-growth-of-autism-in-california
No. Is there a reason too? Jill Escher seems to have not only misunderstood the data, but also my intent. Her piece appears to be an emotional response, as though I were attacking her. This is quite sad. Multiple people at SFASA have my email, including Jill, and could have easily contacted me and asked if I was trying to insult them. I was, and am, pointing out that they are clearly wrong. One does not get to chose one set of data to fit a model and ignore the rest. Or, to be specific, one does not pick only the autism count and ignore ID and claim the rise represents a true increase in the fraction of Californian’s who are autistic.
As noted above, I requested these data before SFASA published their report. Not to rebut their report. I held off for over a year trying to voice this properly and finally decided that trying hard to voice this in a way that would not be seen as insulting. But, frankly, I have to say it–many people and groups can and do misuse these data.
Let’s just stick to facts:
Look at the graph above. Notice the sharp peak in the early 1990’s. That’s not that “growth in this category has declined”, that’s a drop. It is precisely a decline. Rendering the rest of her defense pointless.
Now, let’s get to the important part. Why challenge those (again, SFASA is only one of many) who are wrong here. Is it because after 30 years as a professional researcher, I dislike bad use of data? No.
SFASA is an advocacy organization. They should be advocating for all autistics–even those who are undiagnosed. And there is a large population of undiagnosed adults. There is also a large population of undiagnosed children. Undiagnosed usually means misdiagnosed. And we aren’t talking about people with so-called “high functioning autism” either. People across the spectrum.
We need to be getting these individuals appropriate services. We need to be pushing our legislature and regional centers to identify adults and serve them appropriately. Not only because this is right, but because this will also wake them up to the situation. The current plan is to say that there is an epidemic and there will be a wave of adults coming in the future. This has been the message for over 15 years. Has the legislature done anything? No. legislatures don’t care about problems that will arise in the future. So, not only is this approach based on a bad interpretation of the data, it is also neglecting the needs of autsitic Californians and failing to achieve the stated legislative goals.
The fact that much of the rise in autism in California has already been ascribed to socially driven forces is missing from SFASA’s position. Peter Bearman at Columbia was able to account for nearly 1/2 of the rise with various causes. Irva Hertz-Picciotto at UC Davis found something like 25-30% could be accounted for in the factors they considered.
Many people misrepresent these findings as “they showed that only a fraction can be accounted for, therefore the rest is a ‘real’ increase in autism”. Nope. Just because we haven’t found the explanation yet, that doesn’t mean we get to pick one. At first people said “it’s all real”. They the MIND Center team said, “here are explanations for about 25-30%”. Then Columbia said, “we have even more reasons and we can account for nearly 50%”.
Time and again we see that today we aren’t diagnosing all autistics. Every CDC report has a signficant fraction of the prevalence that comes from children who were unidentified before the CDC team looked at their records. That’s today. Today, across the country, we are missing identifying autistic children. But we are supposed to believe that in the past they not only did it better, but somehow predicted today’s definition of autism. Because that’s what it means to say that the California data are an accurate count of autistics at all ages.
And that doesn’t even account for the fact that autistics have had a very short life expectancy. A recent study showed that average life expectancy was something like age 45.
I could go on. There are so many other ways to challenge the validity of the claim that the CDDS data are a real accounting of autistics in the state. And over and over, the theory fails.
THANK YOU! That makes sense. I had forgotten about the life expectancy issue, that makes a lot of sense. What do you think adults on the lower end of the spectrum are being misdiagnosed as?
Peter Bearman’s study claimed that a large number were diagnosed as having ID only when they should have had ID plus autism.
In the end, though, the point is we don’t know all of what’s going on in these data. And we should be actively trying to understand rather than claiming they are an accurate count on their own.
Many people are not getting appropriate services because they are misdiagnosed. And that is a problem that doesn’t fix itself.
The fact that much of the rise in autism in California has already been ascribed to socially driven forces is missing from SFASA’s position. Peter Bearman at Columbia was able to account for nearly 1/2 of the rise with various causes. Irva Hertz-Picciotto at UC Davis found something like 25-30% could be accounted for in the factors they considered.
Would this be the same 2009 study by Hertz-Picciotto that Jill Escher cited to make to make her case?Has she done a more recent followup study that you might be citing?
Could you post a link to the study by Peter Bearman?
This was what struck me me most from Escher’s article.
Our state has, for example, just 140 45 year-old DDS autism cases, but a whopping 3,196 15 year-old such cases. Did DDS really miss approximately 3,000 45 year-olds with DDS-level autism? Not to mention all the other adults of all ages? The idea is preposterous. No one who works in this system thinks there exists an appreciable number of severely affected adults with autism lurking in the shadows, hiding in basements or attics, or otherwise hidden from our system. These people would have been diagnosed with something in the developmental disability orbit, and likely would have been institutionalized. But at its peak in the 1960s California institutionalized just 16,000 people. We have 300,000 in the DDS system today.
Are there reliable statistics out there that compare how many people were in institutions in the 1960s with those in the DDS systems today?Not just in the US,but in other countries as well.
If you notice, Jill first says that there is no decline, then discusses the decline. She makes basic errors like claiming the decline could be due to selective abortions of Down Syndrome fetuses. Except that DS prevalence has increased. It goes on and on like that.
http://www.ndss.org/About-NDSS/Media-Kit/Position-Papers/CDC-Study-on-Prevalence-of-Down-Syndrome-/
Dr. Carey, do you think this is a valid study? Original Research ARTICLE
Front. Hum. Neurosci., 05 July 2013 | http://dx.doi.org/10.3389/fnhum.2013.00354
Intellectual development in autism spectrum disorders: new insights from longitudinal studies
Giacomo Vivanti1,2*, Josephine Barbaro1, Kristelle Hudry1, Cheryl Dissanayake1 and Margot Prior1,3
1Olga Tennison Autism Research Centre, School of Psychological Science, La Trobe University, Melbourne, VIC, Australia
2Victorian Autism Specific Early Learning and Care Centre, La Trobe University, Melbourne, VIC, Australia
3Melbourne School of Psychological Sciences, University of Melbourne, Melbourne, VIC, Australia
The presence/absence of Intellectual Disability (ID) is considered to be the most critical factor affecting outcomes in individuals with Autism Spectrum Disorders (ASD). However, the question of the specific nature of ID in ASD has received little attention, with the current view being that ID is a comorbid condition (i.e., one that is unrelated in etiology and causality from the ASD itself). Recent advances in developmental neuroscience, highlighting the importance of early exposure to social experiences for cognitive development, support an alternative view; that ID in ASD might emerge as a consequence of severe social-communication deficits on the experience-dependent mechanisms underlying neurocognitive development. We tested this prediction in two independent samples of young children with ASD (Ns = 23 and 60), finding that children with greater ASD severity at an initial assessment were more likely to present with poorer cognitive outcomes at a later assessment, irrespective of initial cognitive level. The results of this proof of principle study suggest that ASD symptom severity contributes to the extent to which the environmental input required to support “typical” brain development can be processed by the individual, so that the risk of developing ID increases as the number and severity of ASD social-communicative impairments increase.
Introduction
I’m coming to this article late (okay, 2 years late), so don’t know how relevant this comment will be. I just wanted to say that I know anecdotally, personally, that the CDDS data is undercounting people with ASD. My child and friends’ children who have been diagnosed as being on the spectrum have been refused services because they are “too high-functioning.” Additionally, children who were diagnosed with ASD under the DSM IV who, for whatever reason, have been re-assessed, but now under the DSM V, have often been given a diagnosis of some communication disorder, thereby rendering them ineligible for CA services.