
Here’s a screenshot from the Age of Autism Facebook page:
I was going to make some comments, but it says a lot just on it’s own.
—
By Matt Carey
Here’s a screenshot from the Age of Autism Facebook page:
I was going to make some comments, but it says a lot just on it’s own.
—
By Matt Carey
There’s a belief I’ve seen recently online claiming that studies from Scandinavia don’t relate to the U.S. because autism is rare there (3 in 10,000) and that autism in Scandinavia is primarily “high functioning”, Asperger syndrome or the like. I won’t link to the discussions as I’ve tried to avoid using the blog to continue discussions found online elsewhere.
I don’t know where this myth originated. But here’s a recent study from Sweden and this result (1.15% autism prevalence, intellectual disability in 42.6%)
The 2007 year prevalence of ASD in all children and young people was 11.5 per 1,000 (95% confidence interval 11.2–11.8), with a co-morbid intellectual disability recorded in 42.6% (41.0–44.2) of cases. We found 96.0% (92.0–98.4) of reviewed case-notes being consistent with a diagnosis of ASD, and confirmed ASD in 85.2% (66.2–95.8) of affected twins.
Yep. Prevalence comparable to the US and with a similar level of intellectual disability.
While we are at it–the prevalence is also pretty much flat for ages 9-18 (kids born from 1989 to 1998) as well.
![plos_sweden_figure_1_top[1]](https://leftbrainrightbrain.co.uk/wp-content/uploads/2014/07/plos_sweden_figure_1_top1.png)
As noted before, thimerosal exposure from infant vaccines was low in Sweden before the 1990’s and was reduced to zero in the early 1990’s. So, for few people still clinging to the “thimerosal epidemic” idea, here’s another nail to add to that coffin.
Another recent study shows prevalence in Scandinavian countries to be between .5 and 1 per 1,000.
—
By Matt Carey
The bill which authorizes funding for the US federal government’s autism research effort expires this September. The re authorization bill is called the Autism CARES Act (Autism Collaboration, Accountability, Research, Education, and Support Act of 2014). The U.S. House of Representatives passed the bill and it passed the Senate HELP Committee. If it passes the Senate and gets signed by the President (pretty likely) it’s a law.
It is now waiting to be brought to the floor of the Senate for a vote.
The last time the research authorization bill was passed (the Combating Autism Reauthorization Act), the reauthorization happened at the last minute: September 30th. A new Committee to advise and plan autism research didn’t start work until the next July. This IACC met for the last time a few weeks ago, so if events go as before it will be a full year without stakeholder input on autism research. If Autism CARES passes soon, the government can start working on a new committee earlier and the delay will hopefully be shorter.
The Senate will go on recess at the end of the week (by law they have the month of August off). So now would be a good time to remind them to bring this to the floor and get it moving.
Autism Speaks has set up a handy web app to help you do this: http://bit.ly/SensCall. Click it, input a little information and it calls you back and sets up the call for you to your senators’ offices.
FaxZero lets you send 5 faxes a day from the web and they have a handy web interface to help guide you to your own (or any other senator). That is http://faxzero.com/fax_senate.php
Want to fax everyone in the senate in one fell swoop? For about $10, http://www.faxyouropinion.com/senators will send the same message to each senator. Don’t worry, they change the “Dear….” line for you.
Want to send those 5 free faxes from FaxZero and wonder who might be someone worth faxing? Well, there’s a set of groups who have been trying to block Autism CARES. These groups set up a list of targeted senators (all these groups are in the “vaccines cause autism” persuasion, 3 directly associated with Andrew Wakefield…yeah, sit back, do nothing and Andrew Wakefield will help shape U.S. autism policy for you. Now that’s a cheery thought!)
Here’s their list. (Their staffs are very nice. One Senator goes straight to voicemail, though).
Senator Rand Paul in Kentucky
Senator Ted Cruz in Texas
Senator Mike Lee in Utah
Senator Tom Coburn in Oklahoma
Senator Roy Blunt in Missouri
Senator Ron Johnson in Wisconsin
Senator Jim Risch in Idaho
Calls only take a minute. You can just call and say, “I’m autistic and I want Autism CARES brought to the floor. Please support it” or “I’m the parent of an autistic kid and I want Autism CARES brought to the floor. Please support it”. Or you can say “Please kill the Autism CARES Act”. It’s your Senate. Use it.
—
By Matt Carey
Note: I serve as a public member to the present IACC, the committee which is authorized by the Combating Autism Act. My comments here and elsewhere are always my own.
The Washington Post has a series of articles about a pair of twin autistic adults who were found locked in a basement room. Here are the first two:
Rockville, Md., couple charged with abusing twin 22-year-old autistic sons
and
Rockville autistic twins who were locked in room are moved
From that second article:
The autistic twins who spent nights locked inside a urine-stained room in their parents’ basement have been safely placed in another home under the oversight of social workers, Montgomery County authorities said Tuesday.
The young men, 22 years old, also have undergone medical checkups, which didn’t find signs of further abuse, police said.
Their parents — John and Janice Land — have each been charged with two counts of abuse of vulnerable adults and two counts of false imprisonment. It appears that the authorities’ case against them rests on the conditions that left the two men inside a filthy, dark room with only an old comforter to sleep on. Neither man can communicate verbally. The doors to the room were bolted from the outside, and the basement also was blocked in places by plywood, according to police accounts and fire inspection reports.
“This case is unacceptable,” said Laurie Reyes, a Montgomery police officier who works with autism families. “There are other measures that can be put in place.”
She said that the conditions for the twins were the worst she had ever heard of in the county.
“the worst she had ever heard of in the county”
Not “just” locked in the basement. Squalor. Filth. According to a later article, the house has been condemned.
This inspired the Post and writer Dan Morse to write another article: Coping with adult children’s autism, parents may face ‘least bad’ decisions
Mr. Morse, I appreciate what you are trying to do. We absolutely need better supports for our autistic adults. But framing this story around the actions of these parents is bad. Really bad. I am at a loss for words in describing just how bad.
I’ll pull one sentence out.
But John Land’s father — John Land III — has said the criminal allegations are overstated given the challenge the twins presented.
If you are going to write that, what about a loud rebuttal? How does being disabled make it non criminal to hold these twins in a squalid prison cell? I frankly think the criminal charges are understated, much as this rebuke is extremely understated.
This sort of abuse can never be the “least bad” choice. Not even close.
Please, find a way to write about the challenges faced–from the perspective of the autistics. Find a way to write about autistics as equals, humans who deserve support because we, the non disabled, should live up to our responsibility.
—
By Matt Carey
Medicaid will start paying for autism therapies. The news was released at the last IACC meeting and I’ve been trying to work out how best to write it since. Seems pretty straightforward, doesn’t it? Not to take anything away from the person who presented it at the meeting but after a while of hearing things like:
Those categories include: section 1905(a)(6) – services of other licensed practitioners; section 1905(a)(13)(c) – preventive services; and section 1905(a)(10)- therapy services.
I just get saturated with the 1915(a) vs 1915(i) type language.
Here’s the announcement: Clarification of Medicaid Coverage of Services to Children with Autism
Here’s one of the first paragraphs:
The federal Medicaid program may reimburse for services to address ASD through a variety of authorities. Services can be reimbursed through section 1905(a) of the Social Security Act (the Act), section 1915(i) state plan Home and Community-Based Services, section 1915(c) Home and Community-Based Services (HCBS) waiver programs and section 1115 research and demonstration programs.
See what I mean? Take from this “the federal Medicaid program may remburse for services to address ASD”
How did this come to pass? A lot of people have been pressuring medicaid for some time to provide autism services. This includes lawsuits, like this one in Florida (Judge: Florida Medicaid Must Cover Therapy for Autism).
If you listen in or watch the IACC meetings, you know that for the past few years one of the sources of pressure on Medicaid has been from IACC member Idil Abdul. I don’t know if a meeting has gone by where Idil hasn’t talked about the inequities of a system where we say we will give medical support to our disabled poor, but we withhold support for treatments related to their disability. Or, to put it simply: why should kids with private insurance get speech, OT and other services while other kids don’t under medicaid?
People often ask what is the value of the IACC and here is one of those unquantifiable benefits. Idil did what a public representative to a federal committee should do: she informed federal members of the needs of the community. Across the table from her was John O’Brien of Medicare and Medicaid Services. John is a good guy and would often patiently correct some factual errors in what Idil had said. But he had to listen to Idil.
And for those of us who know Idil, when I say “she informed federal members” you have to know that “informed” is a major understatement.
Would this shift in Medicaid policy have happened without Idil? It was a big group effort as I’ve already said. Would it have happened later without Idil? We can’t rerun the experiment.
Just to be clear–this wasn’t an effort of the IACC. This was an effort of a member of the IACC. Made possible by her being on the IACC. It’s an odd distinction, but an important one. The structure congress created of the IACC got Idil’s voice in the right place at the right time.
While on the subject of distinctions: as always, my comments are my own and they do not represent the views of the IACC.
—
By Matt Carey
There are many parent advocates asking for research into gastrointestinal disorders and autism. My own anecdotal observations have been that these same parent advocates are of the belief that no work is ongoing. There are a number of projects ongoing and I’ve tried in the past to make that point (What projects are being funded in autism research? Part 1: vaccines and GI issues). I found 14 projects, nearly $3M in 2010. I found 11 projects for $1.7M in 2009.
I thought it time to revisit this question. I’m using a different data source–the NIH RePORTER database. Because of that these projects are those funded by NIH. Other Federal groups can and do fund autism research. Also private organizations like Autism Speaks
Below are the projects I found for the past few years. There are projects on epidemiology, treatment and biology.
While I think that the funding agencies could do a better job informing the communities about these projects, I sincerely wish that the parent advocacy groups calling for this research would inform their members that it is going on. I am actually very curious as to why they have not done that.
MECHANISMS OF AUTONOMIC BRAINSTEM DEVELOPMENT ($243,000)
Brainstem and autonomic circuitry, though understudied in neurodevelopmental disorders, are implicated in pathophysiology and co-occurring medical conditions, such as gastrointestinal disturbances (GID). The goal of this R21 project is to fill this knowledge gap, based on significant preliminary data.
CASEIN KINASE 1 INHIBITORS FOR TREATMENT OF AUTISM $349,610
The overall goal of our program is to (1) identify CK1 [Casein Kinase 1] inhibitors suitable for development as therapeutic agents and (2) to use these agents to investigate the suitability of CK1 inhibitors for addressing specific behavioral features of the complex, multi-symptom disorder known as autism.
The CADDRE SEED studies are multiyear but I haven’t listed all the grants. So the amount is much higher than even the substantial sums noted below.
MD CADDRE: STUDY TO EXPLORE EARLY DEVELOPMENT, SEED PHASE II $91,706
MD CADDRE: STUDY TO EXPLORE EARLY DEVELOPMENT, SEED PHASE II $1,600,000
CALIFORNIA CADDRE-SEED PHASE II $1,100,000
NC CADDRE: STUDY TO EXPLORE EARLY DEVELOPMENT (SEED) PHASE II $1,100,000
COLORADO CADDRE STUDY TO EXPLORE EARLY DEVELOPMENT CADDRE_SEED II $1,100,000
PA-CADDRE: STUDY TO EXPLORE EARLY DEVELOPMENT (SEED) PHASE II $1,100,000
SEED will address hypotheses including: ASD phenotypic variation, including the pattern of clustering of core symptoms, timing of onset, cognitive status, and presence of medical and psychiatric co-morbidities; gastrointestinal features; genetic variation and interaction with environmental risk factors (GxE); infection, immune function, and autoimmunity factors; hormonal factors and maternal reproductive characteristics; and sociodemographic and lifestyle factors.
INVESTIGATING THE GUT MICROBIOME FOR NOVEL THERAPIES AND DIAGNOSTICS FOR AUTISM $558,136 (also funded in 2013 for $558,136)
Based on compelling preliminary evidence, this project aims to explore the potential connection between GI barrier defects and altered behavior in preclinical models of autism. Our long-term goal is to explore possible serum biomarkers for ASD diagnosis, and potentially develop a novel probiotic therapy for at least a subset of children with ASD with GI issues.
2013 projects
TREATMENT OF MEDICAL CONDITIONS AMONG INDIVIDUALS WITH AUTISM SPECTRUM DISORDERS $488,568 (also, $339,591 in 2012, $264,726 in 2011, $578,006 in 2010, $535,209 in 2009, and $465,840 in 2008)
The life-long impairments in communication and social function are often complicated by the presence of medical comorbidities, including epilepsy, (and epileptiform discharges), gastrointestinal disturbances and sleep disorders.
REGULATION OF GASTROINTESTINAL NEUROMUSCULAR FUNCTION BY NIBP/NFKB SIGNALING $320,576 (and 2012 $343,747)
The proposed research is relevant to public health because the discovery of a novel function of NIBP/NFkB signaling in enteric neurons and glial cells is ultimately expected to increase the understanding of the pathogenesis of gastrointestinal diseases. It also shed light on the therapeutics for gastrointestinal inflammation and functional disorders.
ARE AUTISM SPECTRUM DISORDERS ASSOCIATED WITH LEAKY-GUT AT AN EARLY CRITIACAL PER $292,221 (and 2012 $302,820, and 2011 $302,820)
This project seeks to answer fundamental questions about the connection between early development of gastrointestinal (GI) problems (constipation, diarrhea, vomiting, etc.) and autism spectrum disorders (ASD)
From 2011
NEUROIMMUNOLOGIC INVESTIGATIONS OF AUTISM SPECTRUM DISORDERS (ASD) $264,726
A number of anecdotal reports have linked autism with gastrointestinal (GI) dysfunction; most notable among these are reports that autism is associated with “leaky gut” syndrome. Microbial translocation (MT) is the process by which bacteria or microbial byproducts permeate through the wall of the GI Tract (or other abnormally porous mucosal barriers) into the bloodstream. The microbial byproducts would then stimulate the immune system, which could have secondary effects on CNS functioning, or the byproducts could have a direct neurotoxic effect. We conducted assays of MT products in children with autism (from blood and CSF), as well as typically developing children (blood samples only).
and
Our ongoing phenotyping studies will be used to identify a cohort of children with autism who also have significant gastrointestinal symptoms in order to address this potentially important subgroup of patients.
A PRIMATE MODEL OF GUT, IMMUNE, AND CNS RESPONSE TO CHILDHOOD VACCINES $156,634
—
By Matt Carey
Ask someone about autism and Korea and, if you get any answer at all, you will likely hear about the whole population prevalence study that showed 2.64%. What about autism in Korean communities outside Korea? The U.S. has large Korean populations, especially in Los Angeles and New York. And these communities are terribly underserved.
Autism Speaks, George Washington University and the University of Pennsylvania have teamed up with the Korean Community Services (KCS) of Metropolitan New York to create a hotline for autism information.
Two people I respect greatly are involved with this: David Mandel (U. Penn) and Richard Grinker (GWU).
![korean_kids_line[1]](https://leftbrainrightbrain.co.uk/wp-content/uploads/2014/07/korean_kids_line1.jpg)
I’ve copied the part of the Autism Speaks article (the Korean part) below, in the hopes that adding more information in Korean to search engines will result in more people finding the information.
뉴욕한인봉사센터 (KCS)가 오티즘스픽스, 펜실베니아 대학교 정신건강정책서비스 연구소, 그리고 조지워싱턴 대학교의 지원 하에 KCS키즈라인 서비스를 시작하였습니다. 이 프로젝트를 위한 오티즘스픽스의 지원은 블룸버그 가족 재단의 기금을 통하여 이루어졌습니다.
KCS 키즈라인은 자폐(Autism Spectrum Disorder) 또는 발달지체와 관련된 걱정거리를 안고 있는 한인 가족들에게 필요한 정보를 제공하고, 자폐 관련 서비스로의 연결을 돕기 위한 한국어 전화서비스입니다.
오티즘스픽스 공공보건부 어시스턴트 디렉터인 에이미 대니얼스는, “KCS 키즈라인은 한인 지역사회 내 자폐에 관한 인식을 높이고 정보를 제공하기 위한 이전의 노력들에서 한 단계 더 나아가, 자녀들에 대한 우려를 가진 가족들에게 꼭 필요한 정보를 즉각적으로 제공하게 됩니다. 우리는 이 서비스를 통해 가족들이 필요로 하는 도움을 좀더 직접적이고 시기 적절하게 받을 수 있도록 돕기를 희망합니다.” 라고 말했습니다.
미주 아시안 연합 인구조사 센터 (The Asian-American Federation Census Information Center)에 의하면, 한국인은 뉴욕시에서3번째로 큰 아시안 그룹으로 현재 10만명 이상의 한인들이 뉴욕에 거주하고 있습니다. 뉴욕시 교육부는 아시안 학생이 전체 뉴욕시 학생의 16%를 차지하고 있는 것에 비해, 자폐 진단을 받은 아동들 중 아시안은 단 8% 뿐이라고 밝혔습니다. 이러한 수치의 차이는 한인사회 내에서도 자폐 진단이 제대로 이루어지지 않고 있을 가능성을 시사합니다. 오티즘스픽스 재단의 연구비 지원 하에 2011년 한국에서 실시된 자폐 발생률에 관한 연구 결과에서도 비슷한 결과를 볼 수 있었는데, 자폐의 범주 안에 있는 아동 중 2/3가 사전에 진단을 받지 못하였고 적합한 서비스 또한 받지 못했던 것으로 나타났습니다.
한인사회 내에서 자폐 진단이 잘 이루어 지지 않는 이유는 자폐에 대한 인식 부족, 사회적 낙인, 그리고 문화를 고려한 서비스의 부족으로 보이며, 언어장벽 또한 서비스를 이용하는 데에 있어 장애요소가 됩니다. KCS 키즈라인의 목표는 뉴욕시 내 자폐를 가진 한인 어린이들이 빠른 시간 내에 적절한 서비스를 받도록 하는 데 중점을 두고, 그 부모와 가족들을 좀더 효과적으로 지원하며, 궁극적으로는 한인사회의 자폐에 대한 인식을 증진시키고, 자폐 관련 자료들을 많은 사람들이 쉽게 이용할 수 있도록 돕는 데 있습니다.
KCS 키즈라인은 아동의 연령에 제한을 두지 않으며, 주된 대상은 출생 이후 3세까지의 자폐 및 발달지체의 증상을 보이는 아이의 부모들입니다. 부모님이나 보호자들은 전화, 이메일, 또는 방문을 통해 정보를 받을 수 있습니다. 또한, 오티즘스픽스 재단의 지원을 통해 한국어로 번역된 100-Day Toolkit (자폐 진단 후 첫 100일 동안 아동을 케어하기 위한 정보) 및 여러 가지 자폐에 관한 자료들을 오티즘스픽스 웹사이트에서 무료로 다운로드 받을 수도 있습니다: http://autismspeaks.org/korean. KCS는 자폐와 관련된 서비스 자료들을 꾸준히 모으고, 더 높은 연령대의 아동들과 그 가족들 또한 도움을 받을 수 있도록 뉴욕시 내의 학교 및 커뮤니티 기관들과 지속적으로 연계함으로써, 더 많은 한인 가족들이 필요로 하는 서비스를 제공받을 수 있도록 노력할 것입니다.
—
By Matt Carey
A new large study on autism genetics just came out: Most genetic risk for autism resides with common variation. The study is in Nature Genetics, one of the top journals.
The study is the latest in the evolved view of autism genetics. Contrary to political statements made by some groups, autism genetics is not about searching for a single “autism gene”. Here’s a quote from the CNN Blog that makes this clear:
Chris Gunter, an autism researcher at the Marcus Autism Center and professor at the Emory University School of Medicine, says the findings of this study are similar to those reported in other studies.
“There is no one gene for autism,” Gunter said. “Instead there are many different genetic variations which each contribute a little bit to the risk of developing the group of symptoms we diagnose as autism.”
No single autism gene. You might carry one or more genes which are associated with autism and not be autistic. But the more you have, the more your risk goes up. It may be linear: each variant has a “score” and you add them up and if your score is very high, you are autistic. Or it may be nonlinear: some genes in combination may create a greater risk than the sum of their individual risks. I don’t think they understand or have cataloged the genes well enough to say.
The researchers in this current paper are estimating about 60% of autism risk is genetic. Here’s a graphic showing the breakdown of the various risks–different types of genes (common genes that are inherited, rare genes that are inherited, new (de novo) mutations, etc.):
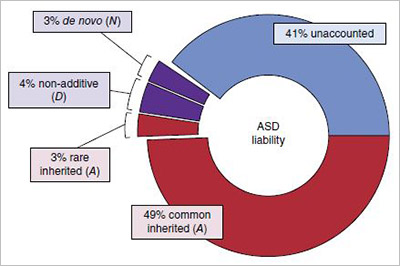
What does this mean for the future of autism research? It means that continuing to look at both genetics and environmental risk factors is valuable. As I’ve said before, from my perspective if autism risk is 10% genetic or 90% genetic, you still need to apply resources to both genetics and environmental risk factors.
Now to answer the more mundane questions. What does this mean for the vaccine epidemic? You can’t have a genetic epidemic (not really true, but good enough for this discussion)! This doesn’t fit with the idea that about 99% of autism is now caused by vaccines.
Yep. These data are yet another reason why your idea doesn’t work.
But isn’t this just blaming the mothers?
I’m always amazed when that argument comes up on autism genetics. And, yes, it does come up. Your children’s genetic makeup is neither a source of pride nor of blame. You really didn’t have any say in the matter. You didn’t create nor change your genes, how can you be blamed for the genes that your child inherits?
Won’t genetic research lead to aborting babies?
Maybe. If it does, it will be much different than the current situation with Down Syndrome. Autism doesn’t have many examples of single-genes, as this study points out. There have already been groups claiming to be working on tests involving multiple genes and autism risk scores.
Does this mean that the story is finished? That we have the last answer about how much risk is genetic and how much is environmental?
No. There will be more papers and more estimates. These are tough questions and knowledge evolves.
Here is the paper’s abstract:
A key component of genetic architecture is the allelic spectrum influencing trait variability. For autism spectrum disorder (herein termed autism), the nature of the allelic spectrum is uncertain. Individual risk-associated genes have been identified from rare variation, especially de novo mutations. From this evidence, one might conclude that rare variation dominates the allelic spectrum in autism, yet recent studies show that common variation, individually of small effect, has substantial impact en masse. At issue is how much of an impact relative to rare variation this common variation has. Using a unique epidemiological sample from Sweden, new methods that distinguish total narrow-sense heritability from that due to common variation and synthesis of results from other studies, we reach several conclusions about autism’s genetic architecture: its narrow-sense heritability is ∼52.4%, with most due to common variation, and rare de novo mutations contribute substantially to individual liability, yet their contribution to variance in liability, 2.6%, is modest compared to that for heritable variation.
—
By Matt Carey
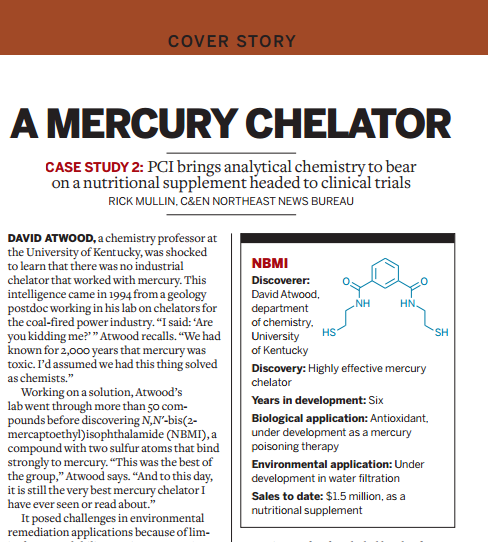
Boyd Haley was a professor of chemistry who was very active in the failed thimerosal-causes-autism movement. He earned extra notoriety for trying to coin the phrase “mad child disease” (yes, a variation of mad cow disease) for autistic children. He also found notoriety for marketing a synthetic chemical as a “nutritional supplement”, calling it OSR#1. Prof. Haley is certainly persistent. He’s working on a clinical trial.
How did this come to pass? Well, one of the professors in Prof. Haley’s department found that a certain compound could effectively treat mining waste, removing mercury. Given his own interests, Mr. Haley started a company with an investor with the intent to bring this chelator to the public. The chelators used in medicine today were developed for lead and have been expanded to also treat mercury. I.e. there is no mercury specific chelator and this new compound would fill that gap.
All well and good, but in his zeal to bring this product to market, Prof. Haley cut a few corners. Chelators are drugs. The compound he was working on was synthetic. But Prof. Haley chose to rush the product to market as a “nutritional supplement”. Instead of calling it a chelator, he called it OSR#1. OSR standing for “oxidative stress relief”. Mr. Haley skipped the process to prove that his drug was safe and effective. Supplements have a much lower standard for safety and efficacy testing.
The FDA was not fooled. Mr. Haley and his company were given a warning letter which pointed out that the compound is not a supplement, it is a drug:
Your firm markets OSR#l as a dietary supplement; however, this product does not meet the definition of a dietary supplement in section 201(ff) of the Act, 21 U.S.C. § 321(ff). To be a dietary supplement, a product must, among other things, “bear[ ] or contain[ ] one or more … dietary ingredients” as defined in section 201(ff)(1) of the Act, 21 U.S.C.§ 321(ff)(1). Section 201 (ff)(1) of the Act defines “dietary ingredient” as a vitamin, mineral, amino acid, herb or other botanical, or dietary substance for use by man to supplement the diet by increasing the total dietary intake, or a concentrate, metabolite, constituent, extract or combination of any dietary ingredient from the preceding categories. The only substance listed as a dietary ingredient on the labeling of OSR#1 is N1,N3-bis(2-mercaptoethyl)isophthalamide. N1,N3-bis(2mercaptoethyl) isophthalamide is not a vitamin, mineral, amino acid, herb or other botanical, or dietary substance for use by man to supplement the diet by increasing the total dietary intake. Further, N1,N3-bis(2-mercaptoethyl)isophthalamide is not a concentrate, metabolite, constituent, extract or combination of any such dietary ingredient. Thus, because OSR#1 does not bear or contain a dietary ingredient as defined in section 201(ff)(1) of the Act, this product does not qualify as a dietary supplement under section 201(ff) of the Act.
Also that the company was making claims that the drug could treat medical conditions and that the labeling was misleading in this regard. Further, that the toxicity was not adequately tested nor reported.
Your website states that” [s]ome reports of temporary diarrhea, constipation, minor headaches have been reported but these are rare and the actual causes are unknown,” as well as “OSR#1 is without detectable toxicity” and “OSR#1® … has not exhibited any detectable toxic effects even at exceptionally high exposure levels.” However, animal studies that you conducted found various side effects to be associated with OSR#1 use, including, but not limited to, soiling of the anogenital area, alopecia on the lower trunk, back and legs, a dark substance on lower trunk and anogenital area, abnormalities of the pancreas, and lymphoid hyperplasia. Based on these animal studies and side effects known to be associated with chelating products that have a similar mechanism of action to OSR#1, we believe the use of your product has the potential to cause side effects, and the before-mentioned website statements falsely assert that the product does not have the potential to cause side effects. Therefore, these statements render your product’s labeling false or misleading. As such, OSR#1 is misbranded under section 502(a) of the Act, 21 U.S.C. § 352(a).
That was in 2010. Prof. Haley and his company are now back, trying to get a clinical trial started on their compound. Essentially, they are trying to do what they should have done in the first place: get proper approval for a drug. An article in Chemical & Engineering News discusses this effort. Actually, it’s part of the cover story, “Building Pharma Molecules”
The story on Mr. Haley’s Company, CTI Science, has contracted with another company, PCI Synthesis, to manufacture the new compound.
The article is, well, a bit of a sales pitch and gets a few facts wrong. There’s a bit of spin on the FDA warning letter, for example:
“The effort to develop the compound as a mercury poisoning therapy accelerated in 2010 when the company received notification from FDA that it couldn’t market NBMI as a nutritional supplement until it underwent the full drug approval process”.
As we’ve just seen above, the compound is not a nutritional supplement at all. It needs the drug approval process because it is a drug.
The CEO of PCI is quoted as stating:
“The main starting material is cysteamine hydrochloride, which is basically an amino acid and found naturally. So it has attributes that could qualify it as a natural product.”
Which was part of the sales pitch for the OSR#1 in the old days and, again, the FDA disagreed. Just because something is synthesized from a natural product, that doesn’t make it a natural product. Otherwise there would be no synthetic products at all. Everything at some level comes from a natural product.
The article discusses how to qualify for a clinical trial the product must meet current Good Manufacturing Practices (cGMP). The article states:
The primary challenge was the removal of impurities to a level that meets cGMP standards
Think about that a moment. Apparently OSR#1 was sold with more impurities than would meet this standard–a standard for food and dietary supplements.
The article notes that, yes, this compound was sold as a product at one time
Sales to date: $1.5 million, as a nutritional supplement
$1.5M in sales. And the only reason it wasn’t higher was because the FDA stepped in. It was only out for about a year, as I recall.
I found this statement interesting, from the Wikipedia page for the compound:
In animal experiments, the amount of mercury in brain tissue was not increased, but also not decreased
So, even if you believe in the failed mercury hypothesis. What exactly were you supposed to get from this compound? I somehow doubt that even the strong believers in the mercury hypothesis think that removing mercury from, say, your liver will cure autism.
It does seem that Mr. Haley and his company are doing some of the right things now. Show that this drug is safe and effective for its intended purpose: chelation. There are some problematical statements that they may market this not as a drug but as a nutritional supplement, which is a non-starter.
—
By Matt Carey
Robert Kennedy is one of the Kennedy’s. He also is known within the autism communities for his irresponsible and flawed “Deadly Immunity” article which appeared in Rolling Stone and Salon.com and which fueled much of the conspiracy theory mindset in a generation of autism parents. That was almost 10 years ago. A year or so back, Mr. Kennedy appeared at the AutismOne parent convention talking about thimerosal again. It’s hard to find a more receptive audience for his message. AutismOne is a staunch supporter of failed ideas like thimerosal and MMR cause autism. AutismOne is also a place that promotes the ideas that one can cure autism by chemically castrating disabled children, or making disabled children drink bleach or take bleach enemas until they pass their intestinal mucosa (which are relabeled as worms) and more.
If readers will indulge me, let me shift to addressing Mr. Kennedy:
While multiple outlets are taking turns pointing out that you have taken a very irresponsible stance on vaccines, I’ll just ask: Mr. Kennedy, did you spend any time looking around AutismOne? If so–why the hell have you not come forward to distance yourself from the junk science that goes on there? Why the hell did you lend your family’s name to that operation? Your family basically built the special education system in our country. The National Institute of Child Health and Human Development is named for a relative of yours. And you are loaning that name to a convention where the keynote speaker abuses autism parents? Have you sunk so low that you are lending your family’s credibility to Andrew Wakefield?
If you were unaware of what AutismOne is, shame on you for lending your name. If you are aware of these goings on, and don’t distance yourself, your stance on thimerosal is the least of your problems.
—
By Matt Carey

Recent Comments