

In 2008 a paper opened up a new area of research in autism risk factors: Autism: maternally derived antibodies specific for fetal brain proteins. The researchers at the U.C. Davis MIND Institute found that for a subset of autistic kids, they could find antibodies in the mothers’ sera that reacted to human fetal brain tissue. Other teams have found similar results, and the MIND researchers have continued to explore this topic.
In the present study, the researchers studied 131 ASD kids and 50 non-ASD controls. 10 of the ASD kids were born to mothers with the brain specific autoantibodies detected in their serum. Autism severity, by their measure, was the same for the two ASD groups. The rate of develpmental regression is the same for the two groups, but strikes me as rather high at 40-50% . Previous studies by this team and others indicated a higher rate of regression in the ASD kids in the maternal-autoantibody group.
Brain volumes were measured via MRI. Most children were tested during sleep. 10 children (all ASD) were tested under anesthesia. Scans were corrected for instrument distortions before volumes were measured. Brain volumes were higher for the ASD kids than the typical kids, consistent with previous results. However, the kids in the maternal autoantibody group had brain volumes even higher than the rest of the ASD kids. The kids in the maternal autoantibody group had brains 12% larger on average than the non ASD kids, while the rest of the ASD group had about 4.4% larger volumes.
The volume differences were not the same over the entire brain:
Furthermore, the frontal lobe was selectively enlarged in the ASD-IgG children relative to other ASD children, and both gray and white matter were similarly affected.
Previous work by the authors indicate the possibility that the autoantibodies themselves might cause brain differences resulting in autism. Their animal model was rhesus monkeys, whose mothers were injected with the autoantibodies.
The authors note there are a number of open questions:
Obviously, several questions remain: What are the brain antigens recognized by the 37/73 kDa maternal IgG autoantibodies, and what is their role normal neurodevelopment? What induces the production of these antibodies in some women but not in others? What is the mechanism by which these maternal autoantibodies alter brain development? Are there processes that could be implemented to block the deleterious effects of the antibodies? Studies are currently underway to address each of these issues and they will undoubtedly shed more light on the role that maternal
autoantibodies may play in ASD and abnormal brain enlargement in ASD.
Another open question they raise has to do with siblings of the autoantibody ASD kids. In specific, since these autoantibodies can persist in the mother’s serum for many years, it is likely that younger siblings are exposed to them as well. If these children do not develop ASD, what is the reason?
The brain volume differences are shown in summarized in this figure:
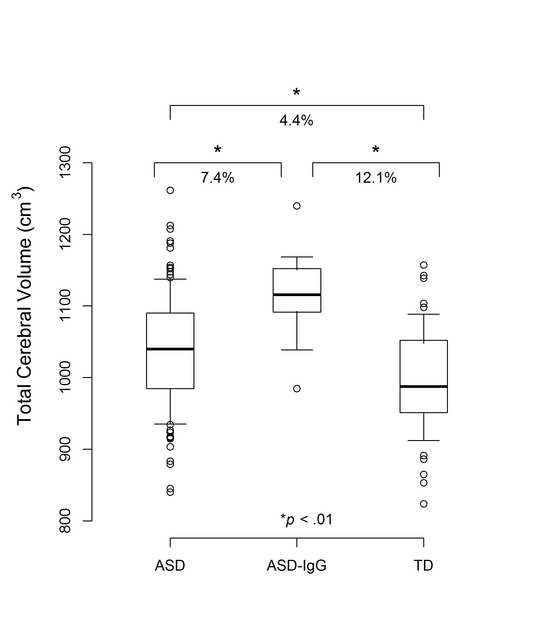
There is a large spread for the brain volumes for the non-autoantibody ASD kids. While on average they are larger, a number are comparable to the average for non-ASD kids. Also, there is a large overlap between the ASD groups from parents positive for the autoantibodies and without the autoantibodies. The kids in the autoantibody group are almost all at the high end of the distribution for the non-ASD kids.
The main thing this paper adds to the autoantibody story is evidence that this may represent a separate group within the ASD population. The work is being performed on members of the Autism Phenome Project. If this is a separate group, so far the evidence is only in brain volume. The authors note: “There were no differences in age, height, autism severity, or DQ between the two ASD groups. Furthermore, the two groups did not differ in the rate of parent reported history of regression.” So on other physical measures, and on autism-based measures, there are no differences. Obviously it would be valuable to see diffrences in autism-specific measures so we could back track how those measures are related to etiology and brain structure. But it is also interesting that this group does not have differences as it could indicate multiple pathways are not always distinct in the end result in autism development.
Nordahl, C., Braunschweig, D., Iosif, A., Lee, A., Rogers, S., Ashwood, P., Amaral, D., & Van de Water, J. (2013). Maternal autoantibodies are associated with abnormal brain enlargement in a subgroup of children with autism spectrum disorder Brain, Behavior, and Immunity DOI: 10.1016/j.bbi.2013.01.084
![]()
—
By Matt Carey






Recent Comments