
Andrew Wakefield recently participated in a cruise/meeting called the ConspiraSea cruise. Among the audience was Colin McRoberts, a skeptic. He reported back during the cruise and, as you will see below, interviewed Dr. Wakefield. Since much of the interview involves William Thompson, Mr. McRoberts asked for my input.
The interview is below. Mr. McRobert’s words are in black, Mr. Wakefield’s in red and mine in green. (If there are any mistakes in that formatting below, they are mine.)
The original interview can be found at An Interview with Andrew Wakefield at
Andrew Wakefield and I were both on the ConspiraSea Cruise in January 2016. By the last full day of the cruise, we’d had a few encounters ranging from standing in the same line for coffee to a fairly tense exchange during one of his lectures. I asked Wakefield after that lecture if he would answer a few questions regarding the so-called “CDC Whistleblower.” He consented, and this is the interview that resulted. Wakefield was aware that I was recording and that I am a critic of his position on vaccines and autism; he did not refuse to answer any of my questions.
This transcript is my own work, and I welcome any corrections. I’ve edited it slightly to make it more readable and remove irrelevant dialog. I have also added parenthetical comments to note where a statement is inaudible on the recording, which is not of high quality, and provide my best guess at what was said in a few places. I have not changed the substance of any question or answer.
Wakefield answered several questions before I turned the recording on. According to my memory and my notes, I asked him questions about the Thompson documents such as what specific deviations there were from the approved study plan (as he had alleged such deviations in two lectures). He referred me generally to his letter of October 2014, written with Brian Hooker and attorney James Moody, and directed to the federal Office of Research Integrity. He indicated both that he had documents from Thompson at the time he wrote that letter, and that Congressman Posey subsequently received additional documents from Thompson. At that point I began the recording.
I am not an expert in the documents Wakefield discussed. So in order to provide context for these answers, we have asked Matt Carey of Left Brain Right Brain to provide commentary. Carey is a published scientist, a parent of an autistic child, and extremely familiar with the Thompson documents. He has written an in-depth analysis of the Thompson documents and was able to provide an important counterpoint to Wakefield’s claims. Please read that excellent analysis prior to this interview if you are not familiar with the affair. The questions and answers will make little sense without context.
My questions are in black, Wakefield’s answers are in red, and Carey’s comments are in green. We welcome your own comments as well.
So the Posey documents that were released are, as far as you know, the documents Posey was given? He hasn’t held anything back?
I think he has probably given Posey more documents than he’s given me. The reason for that is that I’ve just been given the Posey documents, and they’ve been released and they’re available to anyone—you can get them.
I’ve got them.
And I have not been through them as yet, so I do not know to what extent they overlap completely with the documents I’ve got. And the reason I say that is that there may be additional documents he provided to Posey on Thimerosal or other things, because he was involved in two other vaccine safety studies. I have (inaudible: “all the”?) documents relevant to the MMR studies.
The two thimerosal studies were much larger studies and are more significant than the DeStefano MMR study in the evidence against the idea that vaccines cause autism. Given that, it’s interesting that there isn’t much on the thimerosal studies in the Thompson documents. In Thompson’s personal statement he makes no indication that the results of those studies are anything but valid or that the CDC team acted in any way other than ethically in performing those studies.
And then do you know if there are documents you have from Thompson that Posey does not?
I have documents that Posey does not because Thompson and I were in private correspondence.
And when you say that, are they documents that were that correspondence, or were they documents from the DeStefano days?
They are correspondence between us.
So do you have documents from the research or from his work at the CDC that Posey doesn’t have, other than the correspondence?
I don’t know, because I haven’t been through Posey’s documents yet.
One has to ask why he has not yet been through those documents? They’ve been public for some time. I put them online January 4th, nearly 3 weeks before the cruise. A journalist announced he had received the documents from Representative Posey’s office. That was in November of last year. Dr. Wakefield could have submitted his own request then. If Dr. Wakefield felt there was a possibility of evidence of misconduct in these documents, wouldn’t he have read through them at his first opportunity? In his role as creating a documentary about these events, why isn’t he jumping at the chance to add to or confirm his story?
That will answer a lot of my questions, actually. So, Hooker’s study came out, and again, I’m not a scientist—I’m not qualified to review or really have intelligent commentary on a statistical research study. Do you support the conclusions Hooker drew? Do you endorse them?
Do I –
It would be interesting to know what conclusions Dr. Wakefield is thinking of when he responds. There are the conclusions in the paper and there are the conclusions Dr. Hooker has stated publicly since. The last sentence of Dr. Hooker’s retracted study is “Additional research is required to better understand the relationship between MMR exposure and autism in African American males.” That’s quite different from concluding that the study shows a causal link between the MMR vaccine and autism. I believe both Dr. Wakefield and Dr. Hooker have made the latter claim publicly. It is worth noting that an epidemiological study like Hooker’s cannot, on its own, show a causal connection even if the correlation found is strong. The African American males/autism correlation in the Hooker reanalysis is far from strong.
Do you endorse the conclusions Hooker drew in his study based on the DeStefano research?
Yes, I do. I know, and I know you’re going to say it was retracted. It was retracted on the basis that the did not disclose a conflict of interest. There was absolutely no – on the initial basis, the initial rationale for the retraction was nothing to do with the scientific analysis. Which was a very simple analysis, a very simple statistical manip- analysis, which replicated what Thompson found. It was withdrawn on the basis that there was an undisclosed conflict. And that’s why it was withdrawn. There was no undisclosed conflict, and I suspect that there was pressure on the journal to withdraw [inaudible].
First, as I noted above, we aren’t entirely sure what conclusions he stands behind.
As to the retraction, Dr. Wakefield only gives part of the reason why the Hooker study was retracted. Here is the full statement from the journal:
“The Editor and Publisher regretfully retract the article [1] as there were undeclared competing interests on the part of the author which compromised the peer review process. Furthermore, post-publication peer review raised concerns about the validity of the methods and statistical analysis, therefore the Editors no longer have confidence in the soundness of the findings. We apologise to all affected parties for the inconvenience caused.“
The editors were concerned about the validity of the methods and analysis and “no longer have confidence in the soundness of the findings.” That’s a pretty stinging rebuke of the study itself in a retraction and completely avoided by Dr. Wakefield.
But you don’t know that.
No I don’t.
I’ve heard, and again I’m not qualified to even understand the criticism, that Hooker misunderstood how to analyze case control studies. Are you familiar with that criticism?
No I’m not. The criteria for the, if you go to the criteria for the journal, Translational Neurodegeneration, it says papers will be published on the basis of expert peer review. And only when they pass that expert peer review will they be published. The paper went expert peer review which included a statistical analysis and whether he used appropriate methodology. So it passed muster on the basis of the journal’s own rigorous criteria. That gives me cause for concern, because there was nothing in Hooker’s analysis which substantiates or supports the contention that he did not know how to analyze a case control study.
Again, look to the retraction statement by the Journal: Furthermore, post-publication peer review raised concerns about the validity of the methods and statistical analysis, therefore the Editors no longer have confidence in the soundness of the findings. Peer review specifically looking at the statistical analysis found the paper lacking.
I’ve peer reviewed many papers, and even edited the proceedings of a large conference. Some peer reviewers are more rigorous than others. We don’t know what “statistical analysis” Dr. Wakefield is claiming that the reviewer(s) performed. A referee could not replicate Dr. Hooker’s analysis as the data are not in the paper. And datasets like these are not “public use”, they are intended only for those who have shown in their application to be “qualified researchers.” Dr. Hooker should not be sharing the dataset with referees or others.
Also, one question that has been in a lot of people’s minds was who did the first peer review of the paper. Often an author can suggest to a journal potential referees and can use that to get people involved who would be favorable to the authors and/or their conclusions. I can’t say for certain that this occurred in this paper, but it is a possibility.
And of course it’s possible that the peer review was just not very rigorous. A while back a peer reviewed paper included the parenthetical comment, “should we cite the crappy … paper here?” That inappropriate comment made it past referees, editors, type setting, and proofs.
Would it be fair to say that you’ve analyzed the statistical work Hooker did, or –
No I didn’t. I’m not a statistician, although I’ve been involved in a lot of statistical analyses, I would not consider myself an expert in statistics and I am not qualified, certainly over and above the expert who clearly was involved in peer review of the paper, to approve or disapprove of it.
Brian Hooker is also not a statistician. Like many of us in research, Dr. Hooker has some knowledge of statistics, but his own statements (for example, “I reanalyzed the datasets using what’s in a very, very simple statistical technique”) show that he is not an expert in the field.
First, in statistics simple is not always the most valid approach. In this case it certainly is not the most valid approach. Second, and more importantly, this isn’t a statistics study. It’s an epidemiological study. In epidemiology strong studies are those that correct for factors that can lead to false conclusions. Here’s a simple example: rich people can afford healthcare and, as a result, tend to see doctors more often. They are more likely to be diagnosed for many diseases because they seek out healthcare. If a study ignores such factors—takes a “simple statistical technique” it could erroneously conclude that rich people get some diseases more than poor people. Dr. Hooker’s analysis is not only too simplistic statistically, it is too simplistic from an epidemiology standpoint.
Here are two technical critiques of the statistical analysis Dr. Hooker used:
Analysis and Reanalysis: The Controversy Behind MMR Vaccinations and Autism, part 2
Directed Acyclic Graphs and the MMR vaccine doesn’t cause autism
If you’re comfortable saying so, are you still in contact with Thompson?
No. When we – let me qualify that. I write to Thompson. Updating him on our progress. I do not anticipate a response. Because in getting him or encouraging him to get a whistleblower lawyer, his lawyer advised as any good lawyer should that he should make no further comment until a congressional hearing or the equivalent. And therefore I have not heard back from him.
If Dr. Thompson has whistleblower protection, why does he need to only comment in a congressional hearing? The vast majority of whistleblowers are not called before congressional committees.
More to the point, if Dr. Thompson felt that there was ongoing harm—that there was strong evidence of an actual connection between vaccines and autism–he would be ethically compelled to come forward and speak out. In fact, in his public statement Dr. Thompson made it very clear that parents should vaccinate:
“I want to be absolutely clear that I believe vaccines have saved and continue to save countless lives. I would never suggest that any parent avoid vaccinating children of any race. Vaccines prevent serious diseases, and the risks associated with their administration are vastly outweighed by their individual and societal benefits.”
And just to make sure I understand, is that what you understand what his lawyers have told him to do or what you expect his lawyers would tell him to do?
He has said something to that effect in a text. I can’t remember precisely what it is, but he said based upon my lawyer’s advice, I can now have no further contact. So it’s explicitly based on his lawyers.
I’m not surprised. You made a comment that I hadn’t heard before, that it was not true that the data Thompson released showed a protective effect for on-time MMR vaccinations in non-African American male children.
Sorry…
It’s an awkward question. So I had understood that the Thompson data showed a protective effect for on-time MMR vaccinations in non-male, non-African American children. And in your first –
Quite the opposite, quite the opposite. This is the greatest, one of the most misleading things of all, is when the head of science over Autism Speaks, Dr. Wang, was interviewed by Ronan Farrow, that was precisely what he said and what he took from the fraudulent paper. And that underlines just how deceitful the paper was, that the head of science for an organization which is the biggest autism charity in the world, gets it completely wrong when presenting in national media, that giving MMR vaccination on time appears to be protective against autism is the most egregious of all of the sins that they committed.
Dr. Wakefield appears to be misremembering the interview. The Paul Wang/Ronan Farrow interview can be found here. In discussing the DeStefano study, the one that Hooker reanalyzed, Paul Wang stated:
“If you look at children who got the vaccine on time, there is no increased risk.”
Not that there is a “protective effect” but that there is “no increased risk.”
Later in the interview, discussing a different study, Wang mentioned the “protective” effect found. A good discussion of this can be found at Forbes. Allow me to include a few paragraphs from that discussion because it makes an important point about why simplistic statistical analyses can lead to possibly false findings:
Even more surprising was the relative risk among children who had an older sibling with autism: in this smaller group, children with 2 doses of MMR were just 44% as likely to be diagnosed with autism as unvaccinated children. This statistically significant finding indicates, unexpectedly, that vaccines might actually protect children from autism.
The authors were quick to note that there are other good reasons for this apparent protective effect of vaccines: in particular, if parents of autistic children withheld vaccines from their younger children, this could explain the effect. Why? Because we know that autism has a genetic component, and that if one child has autism, his younger sibling is more likely (because they share many genes) to have autism as well. Jain and colleagues explained that if these parents withheld vaccines–because of fears spread by the anti-vaccine movement–then their children could contribute to the apparently lower rate of autism in children who were vaccinated. The authors couldn’t rule out a protective effect of vaccines, but scientifically it seems unlikely, and they wisely offered an alternative explanation.
The “protective” effect is likely an artifact of the study design and the authors acknowledged it. The first thing a good researcher does when she/he finds a result is to challenge it, test it. “If I do a more in-depth analysis, does this finding hold up?” “Is there an alternate explanation that could be causing this and make this result spurious?” Simple is not elegant, as Dr. Hooker asserts. Simple is the first step. And if you don’t take the next steps, your study is weak and your conclusions more likely to be wrong.
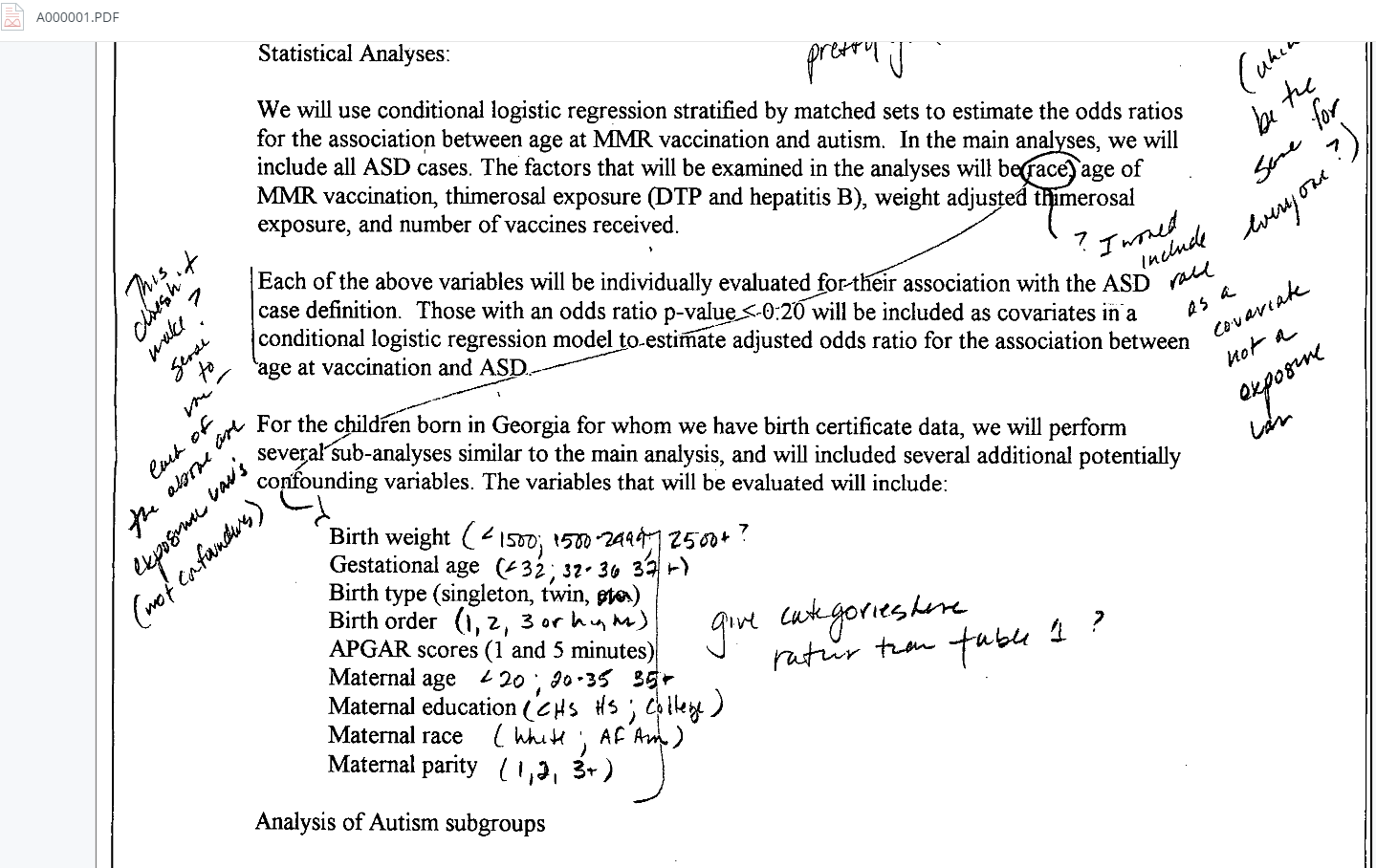
This may also be in the letter you told me to look up, but the destruction of documents—are you aware of specific documents that were destroyed, or types of documents that were destroyed? Or was it just an allegation that documents were destroyed?
Well, what I have are all of the serial outputs of the data covering that period during which the documents were destroyed, and what was quite clear was that the data tables showing highly significant association between autism and vaccination [inaudible: “on time”?] were there before the alleged destruction of documents and were gone afterwards. In other words, the documentary evidence provided by Thompson confirms exactly what he said, that data were destroyed.
This is the story made public in the “garbage can quote” read into the Congressional record by Representative Bill Posey. That can be found in the statement by William Thompson included with the document provided by the Representative to me (and made public by me). Here’s the end key paragraph quoted by Representative Posey. Note that the last line was not read into the record:
However, because I assumed this was illegal and would violate both FOIA laws and DOJ requests, I kept hard copies of all my documents in my office and I retained all the associated computer files. This included all the Word files (agendas and manuscript drafts), Excel files with analysis and results, and SAS files that I used to generate the statistical findings. I also kept all my written notes from meetings. All the associated MMR-Autism Study computer files have been retained on the Immunization Safety Office computer servers since the inception of the study and they continue to reside there today [emphasis added].
Emphasis added. All the files have been retained. If printouts were shredded but the files kept, what’s the controversy? Dr. Hooker and Dr. Wakefield appear to have been claiming that Hooker recreated the CDC team’s analysis solely using the dataset maintained by the CDC and provided upon request to qualified researchers. So, again, what data was deleted?
One might think, well personal notes were shredded and those could show actions that indicate wrongdoing on the part of the CDC team. We don’t know what notes the other researchers retained. But we do have William Thompson’s notes—notes by the person most likely to record wrong doing. We don’t have statements in his personal notes–taken while the study was ongoing–that suggest fraud. In fact one of the few notes that goes to the mindset of the research team states, “we all have good intentions.”
I don’t understand what that means in this context. You have a report of what’s on the servers? Or you have a report of what was in file cabinets? Or you have –
No, I have printouts, or well, sorry, I have email documents. These are documents generated in Word with a date of creation, so that you can confirm that those documents were created contemporaneously with when Thompson said they were created. And they reflect meetings that took place on a serial basis every month, or twice monthly, between the group, the coauthors for that paper. And in September 2002, when Thompson alleges these documents were destroyed, then the African American effect, for example, and the isolated autism effect, were there. And then afterwards, they were completely gone. So that would support Thompson’s contention that documents were destroyed.
The story is much more mundane than Dr. Wakefield is implying here. What is clear in these documents is that this timeframe–around Sept. 2002–is when the research phase of this project ended. Dr. Wakefield tells us, “And then afterwards, they were completely gone.” When you go through the documents you see that after September 2002 there are pretty much no more research group meetings. There were a handful of meetings after this, but the analysis was over and the figures basically finalized. A preliminary draft of the study manuscript is dated Oct. 2002. So the idea that the team met to discuss what to archive and what to shred, and that the figures were finalized about this time is not only not surprising, it’s expected.
And this is where it’s good to have the actual documents. Dr. Wakefield did not share the documents he had, only quotes and screenshots. Bits that supported the arguments he was making. When we see the actual documents we see a different story. When I put up my own analysis of the documents, I made the documents publicly available so people could form their own opinions. From what I can see Dr. Wakefield did not do this.
Speaking of mundane, yes the documents “reflect meeting that took place on a serial basis” as Dr. Wakefield states. In one folder there are about 500 pages of agendas, tables and graphs for those meetings. And when one goes through these documents one finds they are very redundant. The same talking points, the same graphs and tables meeting after meeting. We are asked to be shocked that the CDC team discarded documents. I’ve posed this question publicly–what in those documents needed to be kept? Do we really need multiple researchers archiving every meeting agenda? The answer is simple: no, we don’t. I not only expect them to discard much of this paperwork, I hope they aren’t hanging on to all this paperwork for every project they work on.
I still don’t understand quite what this means. So there was a word document, and in that document, it refers to the African American effect, the isolated autism effect –
It shows the data. It shows the data table.
And in later versions of that document, those tables are gone?
I’ll give you an example. All of the data are contained in a table called Table 5. That table is there in September and it’s gone in October. Never to be seen again.
The last one of these documents– that has “table 5” is, as Dr. Wakefield says, in September 2005. So is Table 8, which includes things like variables “M_AGEC11” and “B_MULTB.” Why is that important? Because those are variable names important to the researchers but were obviously not intended for the final study. The fact that Table 8 (or table 5 for that matter) got cut isn’t a smoking gun, just evidence that these were preliminary tables and that study hit the turning point of finalization.
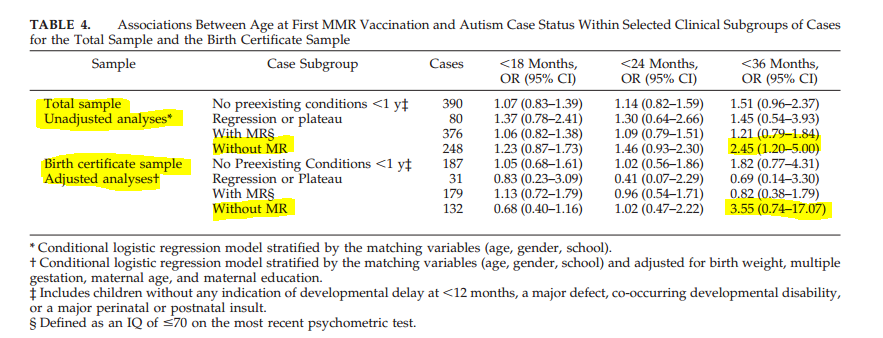
Most of the attention in this discussion goes to the African American effect. Let’s consider the “isolated autism” effect. “Isolated” autism means autism without other disabilities. What happened to that? The CDC team published it. They narrowed it down to autism without MR, but it’s basically the same thing as “isolated.” They also showed that in the simple analysis (the sort that Dr. Hooker claims is “elegant”) there is an apparent association, but that association disappears when one does a more rigorous analysis. Aside from debunking the controversy over “isolated” autism, this serves as another example of why simple isn’t the best.
But the data that was used to create Table 5 – was that destroyed?
Very good question, was the data destroyed. No. No it was not. Because it was not – it was intended to be destroyed. All of the – it was Thompson’s claim that all of the hard copy documents, and all of the computer files, relevant to this paper were targeted for destruction. The original data tables or data files from which the tables were generated were preserved by Thompson and are available and can be reconstructed in order to generate the information. As an example, the data tables – the excel – sorry, they were SAS spreadsheets – provided to Hooker, by which he then did an analysis.
Personally, I want to check the source every time Dr. Wakefield or Dr. Hooker claim to be speaking for William Thompson. Thompson has made very few public comments, plus a few conversations secretly recorded by Brian Hooker and since released by Hooker. Given this, let’s ask ourselves: instead of Dr. Wakefield giving his interpretation of what Dr. Thompson said, why not just quote Thompson? For example, consider the very strong claim “it was Thompson’s claim that all of the hard copy documents, and all of the computer files, relevant to this paper were targeted for destruction.” Now Thompson’s statement, “All the associated MMR-Autism Study computer files have been retained on the Immunization Safety Office computer servers since the inception of the study and they continue to reside there today.”
We don’t know what hard copy documents were kept by the other authors. Or what notes were in notebooks they kept. We hear that they discarded some, but we don’t know that they may have kept. Also, consider this: if “all the hard copy documents” were “targeted for destruction” why meet to decide which documents to shred if the decision is to shred them all? Is it so they can watch everyone discard documents? If so, consider this: we know from Thompson’s own statements that one of the MMR study leaders was missing from the “garbage can” meeting. The story just doesn’t make sense.
We should address the question of discarding research documents: is it unethical? I’ve been a researcher for 30 years. It is common practice to periodically decide what documents to keep in my office, which to archive to a warehouse and which to discard. When I would clear out documents my company would provide me large confidential bins. They look like “garbage cans” except the lid is locked and the only access is through a slot in the top so people can’t fish documents out. After these bins are collected they are sent to a confidential shredder. [Colin: Although I’m not a scientist, I’ve seen similar procedures in very many offices where confidential documents like legal or financial files are used.] I would expect the CDC to have a similar procedure. A researcher keeps the documents that are required to recreate the final analysis and, in my case, determine dates of invention.

As long as we are talking about the few public statements Dr. Thompson has made, allow me to repeat this one:
So that data exists, so far as you know, only in Thompson’s files and not in the CDC’s main files, wherever those may be?
According to Thompson, all of those – he was the only one who preserved all of those records. Beyond that, I do not know the infrastructure of the CDC’s filing system, so I don’t know – I think I’ve probably reached the limit of my knowledge about that. Is there some sort of backup system that retains the original SAS files, I don’t know [inaudible].
“I don’t know.” I believe he should. I see it as ironic that Dr. Wakefield claims to speak for Dr. Thompson (“According to Thompson”) while having not read all the documents Dr. Thompson released to Representative Posey. As I’ve already noted above, Dr. Thompson made it explicitly clear that all the associated MMR-Autism Study computer files have been retained on the Immunization Safety Office computer servers since the inception of the study and they continue to reside there today. At the very least, the raw data exist. Clearly, since Dr. Hooker used those data for his analysis. Also, I’d be curious how Dr. Wakefield knows that Thompson “was the only one who preserved all of those records”. We know that some documents were discarded, but we don’t know what was kept by the other team members.
And then are you referring to statements that Thompson made that have been released, or statements that are still confidential regarding his allegation that those files were deleted?
Both. Both. So his statement to Bill Posey and other documents that I have obtained that are in the documentary. Documents which are not publicly released.
If by the “statement to Bill Posey” Dr. Wakefield means the full statement that Representative Posey excerpted in his House speech, that is indeed publicly released. I released the documents Representative Posey’s office provided to me. I discussed the full statement here.
The full statement is much longer than the excerpts that Representative Posey read. It includes the statement:
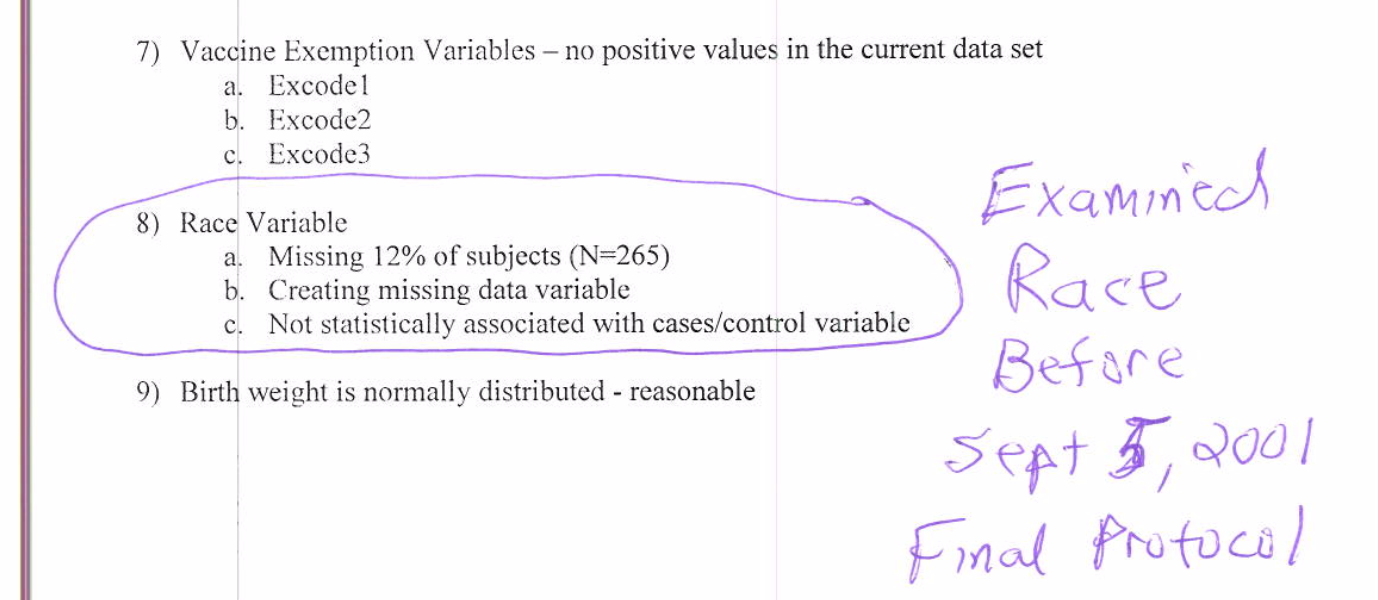
“The fact that we found a strong statistically significant finding among black males does not mean that there was a true association between the MMR vaccine and autism-like features in this subpopulation.”
Emphasis added. I’ll be curious to see if this statement (and others that are problematic for Dr. Wakefield’s story) appear in the documentary.
You mentioned that you’ve analyzed the notes, and that you know who the coauthor was who made some handwritten annotations. Would you disclose who that coauthor is?
No.
Would you disclose how you did the analysis?
No.
Will that be in the documentary?
Yes.
Both the type of analysis and the name of the author?
As yet undecided. [Inaudible: “As yet”?] a matter of discussion.
I was talking to Nick Begich earlier as he dropped these off [pointing to DVDs], and he kind of referred to the breadth of opinions expressed at the conference. And some – I wouldn’t say alarm, but some surprise at some of the views that have been expressed here. And I know that you haven’t been at all the various panels that haven’t involved vaccines or autism, but I think you’ve heard some relatively wild statements. Would you be comfortable establishing a line at which you feel it’s irresponsible to speculate about the cause of autism, or about conspiracies related to medical care?
So sorry, is there a line –
At which you’d object to some of the speculation that’s gone on at the conference.
My reason for coming, or what persuaded me to come, was that Jeffrey Smith was presenting. And Sherri Tenpenny. The other people I don’t know. I’ve met one other person one time. So I know nothing about any of the other people. But I’ve been someone who’s followed Jeffrey Smith for a long time. And I think his approach to his subject is very thorough, is informed, and very valuable. And so every time I get an opportunity to listen to him then I’m very grateful. Sherri similarly. A great deal of knowledge and understanding of the subject. The others, as you say I haven’t been to the talks. I don’t know what their discussions were about.
I am less interested in his “reason for coming” as for why he didn’t consider association with many speakers a reason for not coming.
I’m thinking for example of Len Horowitz’s discussion of the 528 frequency –
Yeah, I didn’t hear that. [Inaudible: “I wasn’t there”?] I just don’t know. So no, I just don’t know. I wasn’t there. So it would be unfair of me to comment on [inaudible].
I heard you speak in Austin, when we were still living there, at an Autism Speaks conference. [I was mistaken; it was an Autism Trust event called the “Give Autism a Chance Summit.”] You were MCing, I think it was Autism Speaks, at the music center downtown in Austin. There were people on the stage like Dr. Kriegsman, and I can’t think of the other guy’s name, who was instructing parents to turn off their routers and their cell phones so the EM waves wouldn’t hurt their autistic children. And I was hoping at the time you would comment to the parents in the room as to whether you thought that was reasonable advice or not, and you haven’t made a statement on it as far as I know. Is that kind of advice something you think is reasonable?
I don’t – if I do not know the subject, I’m not going to give advice. I’m just not going to do it. It’s irresponsible. I’m not going to give advice that could even be potentially construed as medical if I have not done a thorough analysis of the data. Now that said, I keep my mind open to the possibility that there are co-factors that may influence autism risk [inaudible]. I don’t know what those co-factors are. But I’m never going to advise people on what to do based on something about which I know nothing. I’m going to confine myself to the things which I know and I’ve worked on and I’ve read and understood. And where I don’t know I’m going to say I don’t know. If someone has a competing theory of autism, OK, let them talk about it.
One of the reasons my wife and I came to this country is that has a constitution that includes the values we respect. And god forbid that people should be censored or excluded from expressing opinions. Just like the journalists on this trip feeling threatened, that they couldn’t be in discussions, that’s not right, that’s not the way I operate. I encourage dissent because in the end, it’s only through the presentation of competing arguments that truth is going to win. Just in the same way that I talked to you about how it was not our job to censor the parents’ story just because others found it inconvenient or didn’t believe it. It’s not my job to censor other people expressing opinions that may not concur with my own.
I find this highly ironic given the legal threats Dr. Wakefield has made to journalists. He’s even brought suit multiple times against a journalist. A judge in one case referred to Dr. Wakefield’s use of litigation “as a weapon in his attempts to close down discussion and debate over an important public issue.”
Do you feel that given your high profile, your presence might be an endorsement, or at least perceived that way by people who don’t have a chance to talk to you personally?
Well if that is the case, then I should shut myself in a cave on a high mountain, become a hermit. And that’s not going to happen because that’s not the way in which knowledge is going to spread. If people take it as that then it is because they want to take it as that. Because that’s the spin that’s placed on it.
I wanted to ask just one more question.
Go, one more question.
And feel free not to answer. What evidence would change your mind, about a link between autism and vaccines?
What evidence would change my mind… [long pause] What is my position, firstly let’s define what my position is. That’s very very important. Vaccination should operate from a position of an abundance of caution. What you’re doing is you’re taking healthy children and exposing them to a risk or a potential risk. And you’re doing it on the background of the available data on the safety and efficacy of that vaccine. It’s not like you’re taking patients with end-stage cancer, where you say, “Look, you’ve got a fifty percent chance of dying and a fifty percent chance of living, and there may be some benefit but we don’t know.” You’re taking entirely healthy children and you’re giving them an exposure, which incurs a risk. And the risks are all spelled out in the product insert.
So my position, and the position that medicine should be in, is that you operate from an abundance of caution. If there is even a possible risk of harm, then you do everything in your power to either exclude that risk or stop the vaccination policy. First do no harm.
So my position is not that it’s black and white. It is that you operate from an abundance of caution. You have to be very very clear that what you are doing has a minimal, an absolutely minimal risk, for the maximum benefit.
The interesting thing here is the for years the narrative that I recall from his supporters was that Dr. Wakefield didn’t say that vaccines cause autism. He was just posing questions.
That said, see what Dr. Wakefield has done here? He’s framed the question as though there is only one source of risk–vaccinating (and implies falsely that one of those risks is autism). He doesn’t even approach the question of the risk in not vaccinating and leaving one’s self vulnerable to disease. Ignoring that is hardly an “abundance of caution.” Quite the opposite, it’s an abundance of irresponsibility in my opinion.
The positions and the rhetoric that you’ve taken at this conference make it pretty clear you feel that there is extremely good reason to believe that the MMR vaccine in particular, and possibly vaccines in general, and possibly GMOs as well, have a causative link to autism.
Yes.
What would change your mind?
That is because I’ve sat in this field now for twenty years, and nothing has persuaded me that the science is wrong. And what now convinces me that there is a real cause for concern is William Thompson coming forward and saying that a hypothesis that I put forward in the year 2000 is proven to be correct by the year 2001 and was kept concealed for 13 years. How would you feel in that position? Would you feel that it reaffirmed your concern that the parents’ story was right? Or would you think, well, we can dismiss that because – no. It is quite clear that there is a problem they have covered up. So it makes me feel more strongly than ever that we need good, independent science—and I mean independent, independent of the CDC, independent of influence by government or the pharmaceutical industry—that gives us the answers. Will we ever get that? No. We will not get that. Why? Because the system is so distorted, and that’s very very sad. And I’m a scientist, I’ve published 140 papers and I’ve never committed fraud in my life. And I’ve published papers which suggest my hypotheses is wrong. Very few people do that. I publish them. I publish papers – and you can look them up, in the Journal of Medical Virology, saying “we do not find this virus in these tissues.” Despite that being our hypothesis [inaudible]. So I’m perfectly open to the counter-argument. But nothing so far has persuaded me that there isn’t a link, and Thompson’s revelations have reaffirmed to me that there is a link. There is no question, there is a link, they’ve found it. [inaudible] So there we are.
Let’s take on the most important statement here first:
“But nothing so far has persuaded me that there isn’t a link, and Thompson’s revelations have reaffirmed to me that there is a link. There is no question, there is a link, they’ve found it. [inaudible] So there we are.”
But that is not what Thompson says. Again, I’ll quote him directly:
“The fact that we found a strong statistically significant finding among black males does not mean that there was a true association between the MMR vaccine and autism-like features in this subpopulation.”
Thompson doesn’t say there is a link. He doesn’t say “without question.” So, there we are.
Also, it’s worth noting that the above response is worthy of a politician. Ask yourself, did Dr. Wakefield ever answer the question (what would change your mind)? If so, I don’t see it.
If I may, let me discuss the general question of vaccines and autism. I’ve taken this very seriously from the start. This is personal to me in a way that it will never be to Andrew Wakefield as I have an autistic child. I am also a researcher, a Ph.D. I’ve immersed myself in the literature—especially that which claims to show a link between vaccines and autism.
Actually it is Dr. Wakefield’s science, and that of many others who purport to show a link, that showed me that there is no substance to the claim of vaccines being linked to autism. And from that I can say this: it isn’t a question of refuting that claim, it’s a matter of the fact that the claim just isn’t strong at all to begin with.
For example, look at Dr. Wakefield’s conclusion here “Thompson’s revelations have reaffirmed to me that there is a link.” He ignores the bulk of even Hooker’s analysis (most groups show no increased risk of autism) and clings to one small subgroup. OK, that’s a weak stance on his part, but it gets worse. He claims that subgroup result shows not only a correlation, but causation. Even though such a study as this cannot show causation. Even though Thompson himself says this finding “…does not mean that there was a true association.”
There is a large body of evidence, epidemiological and biological, that says that the Wakefield MMR/Autism hypothesis is wrong. But the fact is that the Wakefield MMR/autism hypothesis was never very strong. It’s built on arguments such as “Thompson’s revelations have reaffirmed to me that there is a link.” And, ironically, Wakefield’s work is some of the strongest in the “vaccines cause autism” portfolio.
This post has been edited to restore formatting to the links in Carey’s comments.

{kind=link}
Recent Comments