For a while now, I’ve been hoping that someone would publish data on the current state autism prevalence by birth year in Denmark. Denmark has been used for epidemiological studies for autism since their is a national database for health care. Thus, one can obtain a count of all people in Denmark who have been diagnosed with autism. Which is not the same thing as saying they have a count of all people in the country who are autistic. One can be autistic and not be diagnosed, as we will see.
A recent study using the Danish database is Recurrence of Autism Spectrum Disorders in Full- and Half-Siblings and Trends Over Time: A Population-Based Cohort Study. It’s an interesting study and I feel somewhat guilty for pulling the time-trend data out for my own discussion. In short, the study found that if a family has one child who is autistic, the chance for a subsequent child to be autistic is about 7 times higher than for families without an autistic child. This is fairly consistent with many other sibling studies over the years, but much lower than found in the recent baby siblings study out of the MIND Institute. That might be due to the active surveillance used by the team at MIND. I.e. they were actively monitoring and testing baby siblings.
Much more, they conclude:
Although the results from our comparison of recurrence in full- and half-siblings support the role of genetics in ASDs, the significant recurrence in maternal half-siblings may support the idea of a contributing role of factors associated with pregnancy and the maternal intrauterine environment. Finally, the lack of a time trend in the relative recurrence risk in our data suggests that the likely combination of genetic and environmental factors contributes to the risk for ASD recurrence in siblings or that the risk for recurrence because of such factors has not been affected by the rise in the ASD prevalence.
Very interesting–whatever is behind the higher prevalence among younger siblings, it seems to be the same today as 30 years ago.
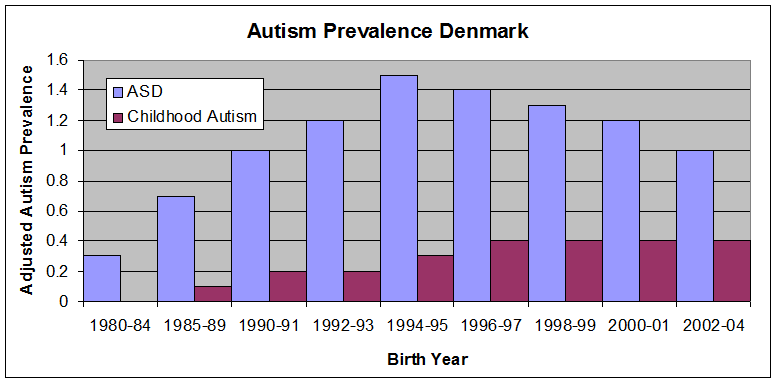
What’s the overall prevalence of autism in Denmark according to this study? For childhood autism, they report 0.3%. For all ASD’s, 1.2%.
Autism, we are told by those promoting the autism/vaccine link, is unmistakable. Each autism prevalence report is not an estimate, but an accurate count of every autsitic because there is no way to miss an autistic. Back in the day, Rick Rollens was a constant fixture in the news on autism. He was a strong proponent of the idea that one could not miss autism:
WATSON:
Like many parents, Rick is convinced that Russell was damaged by a series of vaccinations. He strongly rejects the idea that the epidemic of autism can be entirely explained by poor diagnosis in the past because numbers have rose over the last few years.
ROLLENS:
Missing child with autism is like missing a train wreck. For us now to now think that somehow we have better identified a child who can’t talk, who has repetitive behaviour. Who makes no eye contact. Who is self- involved and in many cases self-abusive just defies logic.
Mr. Rollens was wrong on two counts (leaving aside his inflammatory and derogatory language). First, autism is not just the child who can not talk, self-involved and self-abusive. Second, yes, a lot of autistics have been missed. We’ve seen that time and time again. Look at the same population at different times and the later study will have found more autistics. An this goes for autistics with intellectual disability, as shown in the recent UCLA/Utah autism followup: “Today’s diagnostic criteria applied to participants ascertained in the 1980s identified more cases of autism with intellectual disability. ”
But, what about Denmark? A study from 10 years ago looked at autism incidence following the removal of thimerosal in Denmark in 1992. Thimerosal and the occurrence of autism: negative ecological evidence from Danish population-based data
In that study they found 956 children born in their study period who were diagnosed with autism by 2000:
A total of 956 children with a male to female ratio of 3.5:1 had been diagnosed with autism during the period 1971–2000.
The current Denmark study included individuals diagnosed until the end of 2010. I.e. there were 10 more years of followup. In those 10 years a lot more people were diagnosed. Where there were 956 diagnosed with autism by 2000 (for birth years 1971 to 2000), 2321 were diagnosed by 2010. That’s an increase of 240%. And the new study focused on birth years 1980 to 1999. I.e. the entire 1970’s birth cohort is not included in this count, and they still found over twice as many autistics. Where were they in 2000, when the previous study was performed? Living in Denmark, not identified as autistic.
There are a few factors which are likely behind this increase, but here we have a great example of “increased awareness” affecting autism prevalence.
And, those numbers were for childhood autism. For ASD, the increase is even larger. 10,377 Danes had an autism spectrum disorder diagnosis (for birth years 1980-1999) in the new study (the previous study included none). That’s a whopping 1080% increase. Again, there are a few reasons for this (including the increased awareness above), but here’s what “expanding the definition” does to autism.
Those increases would be an “epidemic” to some if it weren’t for the fact that those autistic Danes were there all along. They just weren’t diagnosed in 2000.
For many years, groups touting the idea that vaccines cause autism have pointed to Denmark as part of their argument. Denmark uses fewer vaccines than the U.S.. Generation Rescue used to have this on their website discussion of vaccines:
Comment: Denmark is a first world country based in Western Europe. Their schedule appears far more reasonable than ours. They have also been reported to have a much lower rate of autism than the U.S. Do they know something we don’t?
What was that Danish vaccine schedule that Generation Rescue recommended?
DTaP at 3, 5 and 12 months
Hib at 3, 5 and 12 months
IPV at 3, 5 and 12 months, plus 5 years
MMR at 15 months and 12 years
No mercury (Denmark phased that out in 1992). No birth dose of Hepatitis B. Fewer vaccines overall than in the U.S.. And the same autism prevalence of about 1%.
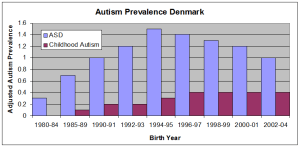
If you dive into more details, it gets even worse for the vaccines and/or thimerosal cause autism argument. Let’s look at the prevalence as a function of birth year for childhood autism and ASD from the recent study:
Consider this statement from a previous study:
This means that children who followed the full vaccination program during the period 1961–1970 had received a total of 400 �g of thimerosal or 200 �g of ethyl mercury by the age of 15 months and during the period 1970–1992 they had received a total of 250 �g of thimerosal or 125 �g of ethyl mercury at 10 months of age. In March 1992 the last batch of thimerosalcontaining vaccine was released and distributed from Statens Serum Institut in Denmark.
The thimerosal exposure was higher prior to 1992 than after. But the prevalence of both childhood autism and ASD is higher after the removal of thimerosal. This is the same result as shown in the 2003 study. The number of vaccines seems to be constant over this time period, so number of vaccines/aluminum/too-many-too-soon or other arguments don’t work either.
How about taking just a single year. The prevalence for ASD in 1996-97 was 1.4%. What is the autism prevalence in the U.S. for that year? To answer accurately, I’d contend we need a count today, not an old one. But people promoting the idea that vaccines cause autism take the CDC reports as absolute measures of autism, comparing each report and telling us all about the epidemic. So, let’s take the CDC number for kids born in 1994: 0.8%. That study was reported in 2009.
So, we have 1.4% in Denmark and 0.8%, nearly half the Danish prevalence, in the U.S.. Denmark had no thimerosal, no Hepatitis B shot (birth or otherwise), fewer vaccines and less aluminum exposure. And much higher reported autism prevalence.
Oddly enough, even though there have been many prevalence studies out of Denmark, Tomljenovic and Shaw didn’t include Denmark in their study “Do aluminum vaccine adjuvants contribute to the rising prevalence of autism?” My guess is that Denmark didn’t fit their conclusion then, and, like Iceland, would make their analysis fall apart now. It is even more odd that Tomljenovic and Shaw didn’t use Denmark as Denmark was used in a faux-study put out by Generation Rescue. In AUTISM AND VACCINES AROUND THE WORLD: Vaccine Schedules, Autism Rates, and Under 5 Mortality Someone at Generation Rescue made the first attempt at the sleight of hand of comparing the autism prevalence in various countries vs their vaccine schedules. At that time, 2009, Generation Rescue claimed that the autism prevalence in Denmark was 1 in 2,200, misrepresenting the 2003 study discussed here. The raw prevalence in this 2008 study was 0.65% or about 1 in 153. That value didn’t fit the thesis that the Generation Rescue author wanted to convey.
One argument found on the internet is that the 2003 Denmark paper fudged the results by clipping the last years off the data presented. An email involving people involved in the study is quoted as saying, “But the incidence and prevalence are still decreasing in 2001“. Oh, my, we are told, the autism prevalence and incidence actually went down after the removal of thimerosal!
But, it didn’t. The prevalence of childhood autism (basically what was studied in the 2003 paper) in Denmark is flat from birth cohorts 1996-2004. Flat. The prevalence of ASD’s do see a decline. That must be it! Evidence that thimerosal was causing autism in Denmark! But it isn’t. The prevalence of ASD in 2003-04 is the same as that in 1990-91, before thimerosal was removed. Why does the ASD prevalence go down? We can’t say for sure, but my strong suspicion is that it’s the same reason why the authors in 2003 were seeing a decrease: too few years of follow up. Autistic kids are typically diagnosed earlier than those with other ASD’s, but the average age was about 5 in Denmark in 2003 (as I recall). ASD kids can have an average age of diagnosis of 8. Recall that the recently released study followed kids up to the end of 2010. It’s no surprise to me that the estimated prevalence for ASD kids born in 2002 is lower than that for kids born in 2000 in this study. And this is consistent with the flat prevalence for kids with childhood autism diagnoses, as they are typically diagnosed earlier and 8-9 years would be enough to find the majority of the autistics in that population.
What about the idea that there’s a “changepoint” in the autism prevalence in Denmark and California pointing to some event in the late 1980s that’s contributing to autism prevalence? For one thing, the present study notes that the recurrence risk doesn’t change with time, so that’s good evidence against such an idea. There is no changepoint in the California data in the 1980’s, as it is exponential and fitting it to two straight lines is just a mistake. What about the prevalence data just released? The data are not finely spaced in birth years, in my opinion, to give a good idea of any “changepoints” in the 1980’s. But there is a changepoint of sorts in the childhood autism data in the 1990’s. The data plateaus at about 1996. But, as already noted, this doesn’t coincide with anything related to vaccines. The ASD prevalence appears to peak at about 1994, but, again, this doesn’t coincide with vaccine events and, I suspect, results largely from lack of follow up for the kids in the later birth years.
How about the MMR vaccine? MMR uptake for young children (MMR1) was basically flat from 1987-1997. Uptake rose somewhat after that. So, during the period that the estimated prevalence was increasing, MMR uptake was basically flat. During the time that the estimated prevalence was either flat (childhood autism) or decreasing (ASD’s), the MMR uptake was increasing. So if we were to play the “correlation equals causation” game, MMR prevents autism. (two notes, preventing rubella infections most likely does prevent some autism and the link above shows a nice example of rubella infections going down after MMR was introduced in 1987. The two points are not linked because most women in Denmark who were infected with rubella before 18 weeks gestation chose abortion, resulting in a low congenital rubella syndrome prevalence).
How about the “fetal cells in vaccines cause autism” argument? It’s one without biological plausibility, but then so was the thimerosal idea. I’d be interested in seeing how the vaccines were produced in Denmark in the 1990’s, but at present, the MMR vaccine there is developed using chicken eggs, not fetal cell lines. And they don’t routinely vaccinate against chickenpox, another vaccine in the U.S. using fetal cell lines. It looks like at least as far back as 1999 they were using egg-based vaccine production for MMR.
So, it appears we have a country with no vaccines grown in fetal cell lines with an autism prevalence as high or higher than that in the U.S.. In other words, the “vaccines from fetal cell lines caused the ‘autism epidemic’ theory” also appears to be debunked by the Denmark data.
In case you are looking for correlations with the vaccine program, here’s the history in Denmark.
So, how about the rise in estimated prevalence in the 1980’s. Is it “real”, as in does it represent an actual increase in the fraction of autistics in the population? It’s a good question and one which could be answered by performing a real study of autism prevalence in adults. The sort of study I and others have called for in the U.S., but that most autism-parent advocacy groups have refused to support. Such a study would not only answer the question of the prevalence, but it would give us valuable data on what has led to success and failure among the autistic adult population.
For those promoting the idea that environmental mercury emissions are a factor in the increase of autism rates, if you have data for Denmark, I’d love to see it. In the U.S., environmental mercury emissions dropped by over 50% in the 1990’s.
Lastly, let’s discuss a comment statement one will read or hear. It goes something like “the autism prevalence was 1 in 10,000 in 1980 and it’s 1 in 1,000 today”. This involves a number of sleights of hand. First, the autism prevalence wasn’t 1 in 10,000 in 1980. It was a few in 10,000 (Wing and Gould reported about 5/10,000). Doesn’t sound like a big deal, but when people start taking ratios (it went up a gazillion percent) a factor of 2 or 3 in the denominator makes a difference. Second, this was the estimated prevalence based on the number of autistics diagnosed at the time. As shown above, the childhood autism prevalence estimate for Denmark in the 1980’s increased by 240% in the past decade. This was not a real increase, but better identification. Third, the comparison is between autism (childhood autism, DSM-III autism or some other restrictive definition) vs. autism spectrum disorders. Also shown above was that the prevalence of ASD’s in the 1980’s increased by a factor of 10, increasing only in the past 10 years.
A factor of 10 in the numerator, a factor of 3 or 4 in the denominator and pretty soon you are talking about a big part of the increases observed.
In the end, none of the above arguments are that new. Or, to put it better, none of the vaccines-cause-autism arguments had much real support. The mercury idea has lost much of the support it had 10 years ago in the parent community, but it persists. The aluminum in vaccines idea has risen to try to take the place of the mercury hypothesis, but it is based on the exact same smoke and mirrors. The idea that the increase in autism is due to the MMR has been scientifically dead for years. And, yet, these ideas persist. And they cause harm, both to the community at large and to the autism community.
—
Matt Carey


Recent Comments