Below are a selected list of discussions about Brian Hooker’s recent paper and the highly irresponsible way he and his team are promoting it. Let me know if you spot one I should add to the list.
Here on Left Brain/Right Brain, I have discussed this as:
One will certainly find more articles, especially searching for the names of the people involved and terms like “CDC Whistleblower”
So far none of the groups who promote autism as a vaccine-induced epidemic have stepped forward to distance themselves from Andrew Wakefield and Brian Hooker’s disgusting race-baiting attack. I hope that will change.
This article has been removed from the public domain because of serious concerns about the validity of its conclusions. The journal and publisher believe that its continued availability may not be in the public interest. Definitive editorial action will be pending further investigation.
I wish they had thought this through before publishing it. Be that as it may, my own view (as an author and one-time editor) is that the revelation that this is not an original work by Mr. Hooker should have warranted some action. Mr. Hooker has discussed how the idea to do this study came from someone else and the analysis is a recreation of a previous analysis. Minor point, I know. And I know my online friends did not agree with me on that.
I do appreciate the journal taking this step. While Mr. Hooker, Andrew Wakefield and their team try to make as much political hay out of this paper as they can.
The groups promoting vaccines causing autism have been handed probably their biggest story in a decade. They are claiming, and it seams likely, that a senior CDC epidemiologist came to them with information that a statistically significant result of possible increased autism risk from the MMR in a specific subpopulation was not reported.
I’ll go into a lot of background below, but if you wish to read up about these events:
Here’s the press release for the recent reanalysis study
Even with multiple press releases and no doubt other efforts to gain media attention, this story has yet to break out into a mainstream news story. Some alternative news sources and many parent supporters of the vaccine/autism idea have discussed this lack of media attention. And there’s a YouTube video by Andrew Wakefield that I’ll embed below. That video deserves and probably will get it’s own article here on Left Brain/Right Brain. It is remarkably bad.
It has often been said that the parents promoting the idea that autism is a vaccine-induced epidemic are their own worst enemies. As the parent of a multiply disabled autistic child I can say without reservation that these groups are no friends to the majority of the autism parent community either. Nor are they friends to the real majority of our community: autistics. The vaccines-caused-an-autism-epidemic parents have refused to support any research which goes against their idea that autism is a vaccine-induced epidemic. They don’t support research into the prevalence of autism in adults. Likely because they worry that this will show that their epidemic idea is false. In the process we lose the chance to learn from the previous generations of autistics about what has worked and what has not. Information which is critical to this autism parent. These groups have failed to accept that the lower prevalence of identified autism in racial and ethnic minorities indicates that the prevalence numbers we so often hear are not the a true count of the fraction of our population that is autistic. Because to admit that is to admit that they are misusing the numbers they rely upon to claim an epidemic. Their lack of support has hindered attempts to improve identification and get appropriate services for autistics in racial and ethnic minorities. This is a point that is incredibly ironic given the way these groups are framing their recent news as you will see (or have seen if you read Ms. Ditz’ article linked above). On top of this they have produced a way over-the-top PR campaign about their news, demonstrating their deep hatred for the CDC. If I were to tell you that Andrew Wakefield is claiming that the CDC are worse than Adolf Hitler, Josef Stalin and Pol Pot (because, you see, in Mr. Wakefield’s eyes at least those dictators were sincere), would you believe me? Would you think I was making this up? If I said that Mr. Wakefield has played the race card in a disgusting way, claiming that the U.S. vaccine program is a new Tuskegee experiment, would you believe me? You can skip down to the bottom if you want to see that discussion and video. I’ll start with the science.
About 10 years ago a team from the CDC published a study: Age at First Measles-Mumps-Rubella Vaccination in Children With Autism and School-Matched Control Subjects: A Population-Based Study in Metropolitan Atlanta (full paper here). They took data from the CDC’s Metropolitan Atlanta Developmental Disabilities Surveillance Program (MADDSP). In order to control for potential confounding variables–like mother’s age, birth weight and more, the authors of the MMR follow-up study pulled birth certificate records. They only pulled them for kids born in Georgia. Could be there was a logistics issue (trying to track down records across the country) or if birth records were not consistent across the US. Also, they would have had to find control kids for those born outside Georgia, and that would have been a big logistics issue. In the end there were two analyses presented–one on the raw data with all the kids, and one with a more detailed analysis done with this smaller “birth certificate” cohort.
This is a good table to review this study. What did they find? The general result is that time of MMR vaccine receipt was similar between autistic kids and non autistic kids, but was statistically more common among autistic kids. In the table above we see that for the most part, the sub groups reported had generally no increased risk of autism with MMR. I.e. in most examples the 95% confidence intervals encompass 1. The unadjusted sample “all cases” and “boys” do not encompass 1. If those were all the data we had, we’d say “let’s look more closely at these”. We’d start with exactly what the authors do–check for confounding variables and see if the effect gets bigger or smaller. In the adjusted data, all the odds ratios encompass one. Some are high enough to warrant a closer look: kids aged 3-5 and boys. Combining these two I’d probably ask, “what about boys aged 3-5”, but the authors take on the age 3-5 question in general in the discussion citing that the 3-5 age group autistics were mostly in special ed preschool and were thus required to have MMR.
If you look at Table 5 (click to enlarge) you see an interesting and very strange trend. It was in the other data but it’s really clear here. The odds ratio is much larger for kids who got MMR before 36 months than for kids who got it before 24 months. The odds ratios still encompass 1, but there is something going on in the data for the kids who got vaccines between 24 and 36 months. And by “something going on” we always have to consider social factors. But take a look:
Take, for example, maternal education. Kids with mothers who had more than 15 years of education had an odds ratio of only 0.61 if their kids got the MMR before 24 months, but that odds ratio jumps up to 2.76 if their kids got the vaccine before 36 months. In both the confidence intervals encompass 1, so we can’t say “MMR before 24 months is protective but MMR before 36 months increases risk”. But that difference is striking. Even if these results were statistically significant, it doesn’t make sense to say, “the MMR vaccine causes autism in kids when it is given between 24 and 26 months if their mothers are well educated. And, by the way, it’s protective if given before 36 months.”
While not as striking, the differences between the unadjusted and adjusted analyses in table 3 are notable. Odds ratios change when you take into account other factors. I’m no epidemiologist, but if this isn’t covered in epidemiology 101 I’ll be stunned. In physics (the field of my Ph.D.) we talk about “hidden variables”. You see one thing correlated with another but in reality a third, “hidden”, variable is actually causing the association.
That said, the CDC MMR paper is not a study without limitations (no study is). One major limitation was the need discussed above–to argue why the 3-5 age group kids had a higher prevalence.
At this point researchers (both the study authors and those reading this paper) and advocates can take a number of approaches. Here are 4:
1) They can say, “yep, that’s plausible enough. We’ve worked this dataset enough. This tells us that MMR doesn’t cause autism. Let’s move on from MMR.”
That didn’t happen and rightfully so. This isn’t a particularly strong study. It’s not the final word and I don’t think it was intended to be. It was a relatively quick study using an existing population. In the end there were more studies on autism and MMR.
2) Advocates and researchers could take the approach: “There’s an association there, but these data are too limited to really answer the question of causation. Can we do a study to nail down if there’s something about those kids born in those specific years (the 3-5 year olds) who got the MMR between 24 and 36 months? Maybe look at further subsets?” And, while it’s easy to say with hindsight, this is the approach that should have been taken in my opinion. I am unaware of work by this team of researchers or external researchers which addressed this question. I am also unaware of calls by the autism community to do such a follow up, by the way.
3) Advocates and/or researchers could say, “I think we can tease more out of these data. Hey, CDC, can I have that dataset to review myself?” Because the CDC did make these data available for serious researchers to review. CDC researchers moved on to other topics in autism and vaccines, but other researchers or qualified advocates could have taken this up.
4) Advocates (not so much researchers I suspect) could say, “I don’t trust the CDC to add 1 and 1. Give me those data and I’ll do the analysis myself. Even those areas where you show a lack of association are probably wrong.” And, yes, there are advocates like that. Well, except that no one asked for the data back then. More recently, though someone did. Which leads us to:
An autism parent and strong proponent of the failed mercury hypothesis, Brian Hooker, recently published a study re-analyzing that old CDC dataset on MMR and autism. His financial backers put out a press release claiming that not only does this study show that vaccines cause autism in a specific subgroup, but that this study was prompted by a CDC “whistleblower”. I.e. someone who was inside CDC and knew about the details of the CDC study was in contact with Mr. Hooker.
That’s a pretty dramatic press release. Let’s take some time on it.
Focus Autism Releases Findings on 2003 CDC Autism Study – Higher Autism Rate Among African-American Boys Receiving MMR Shot Earlier than 36 Months
Focus Autism releases their findings of a possible reduction in the sample size of a major 2003 study conducted by the Centers for Disease Control and Prevention. This sample size reduction negates statistically significant findings from the study.
This title is why I jumped to the press release before talking about Mr. Hooker’s paper. With this title we know (a) that Mr. Hooker is claiming an association among a specific subgroup only (African American boys) and (b) he’s claiming that there was some sort of sleight of hand by the CDC where they reduced the sample size.
Well we already know from the CDC study that autism rates were higher in kids who got the MMR before 36 months. It’s right there in the conclusion statement of the abstract. But not so much before 24 months. And we know autism rates were higher in boys. We didn’t see the analysis narrowed down to African American boys.
The press release states:
“However, CDC researchers did not include any children that did not have a valid State of Georgia birth certificate – reducing the study’s sample size by 41% . Dr. Hooker explains that by introducing this discretionary criteria into the analysis, the cohort size was sharply reduced, eliminating what would have been a higher statistical finding. ”
This is a rather odd statement. And by odd, I mean so obviously false that I wonder why it was written. See for yourself above, the study includes *both* the group with the birth certificate data and the raw data. Mr. Hooker’s explanation is, well, lacking. Sure, it is “discretionary” to try to account for confounding variables. It’s the sort of discretion I expect from epidemiologists. It’s like saying, “the engineers designing the Tacoma Narrows bridge decided against including the discretionary criteria of wind”. Also, consider that a result can be both statistically significant and wrong as is often the case when one finds something “statistically significant” without looking for or correcting for hidden variables.
In another press release Mr. Hooker calls the birth certificate data “irrelevant and unnecessary”. Again, why put out statements that anyone familiar with epidemiology would know to be false?
Elsewhere Mr. Hooker has even challenged the fact that one can obtain the stated data from birth certificates. He is in effect stating that not only is there no point in controlling for such factors, but that the CDC just lied and didn’t even have those data from the birth certificates.
Despite your assertions and the assertions of Destefano, Birth Certificates do not contain the information on the covariates you cite: birth weight, maternal age, maternal education, parity, etc. If you had read my paper, you would see that I repeated the analyses of the CDC and obtained the same results that they obtained in both what was published originally and what was withheld. Also, the birth certificate restriction was NOT applied to other race categories outside of African Americans.
Readers interested in whether Mr. Hooker is correct can take a look at the U.S. Standard Certificate of Live Birth. While this is the revised version, states standardized on birth certificates back in the 1990’s.
Epidemiologists are aware that the piece of paper a parent takes home isn’t necessarily the same birth certificate data that is in the full record.
And “Also, the birth certificate restriction was NOT applied to other race categories outside of African Americans”. Here we see the race card being played. A card that we will soon see was played with a very heavy hand. But to address the assertion made by Mr. Hooker, I wonder how he explains that there are 333 white autistic kids in the “total sample” and 199 in the “birth certificate sample”. Which is to say, his statement is false.
In one of the press releases, Mr. Hooker states
When asked if there could be any scientific basis for excluding children born outside of Georgia, Hooker responded, “I know of none, and none has been provided by the authors of the DeStefano study.”
Again, children born outside of Georgia were not excluded as Mr. Hooker asserts. Analyses were presented on both those born within Georgia (including adjustments for vital statistics found on the birth certificates) and a total sample including those born outside Georgia (the unadjusted analysis). If Mr. Hooker is “unaware” why people would do such an elementary epimiological task as adjusting data with covariates, I suggest he was a poor choice to perform Focus Autism’s study. Another thought would be that Mr. Hooker could read his own paper where he states:
It should be noted that a recent publication has shown that the prevalence of autism in African Americans is nearly 25% higher than that of whites. This value was obtained when CDC data were appropriately analyzed based on socioeconomic status
Mr. Hooker notes that when one does an analysis “appropriately” one includes socioeconomic status (such as with data found in the full birth certificates).
If Mr. Hooker would like to ask why the CDC team didn’t look for birth certificate data on kids born outside of Georgia, that’s would be a better place to start. Then we can discuss whether the CDC would then need 3 controls for each non-Georgia born kid, controls from the same place of birth as the study team did with Georgia born kids. And we could discuss how difficult that would be. And whether that would introduce more problems than it might solve. That’s a reasonable discussion. Claiming there’s no reason to gather important data is not.
Enough of the inconsistencies in Mr. Hooker’s recent statements. What was Mr. Hooker’s method and what did Mr. Hooker find in his analysis? The Poxes Blog and epidemiologcal.net discuss this with more expertise than I can. Mr. Hooker does not recreate the CDC’s case-control study. That would require that match autistic kids and non autistic kids on the parameters he says aren’t available, and adjust for those same parameters. Instead he does a cohort study without adjustments. As discussed elsewhere, this is a much weaker approach. His main result is as the press release states “Higher Autism Rate Among African-American Boys Receiving MMR Shot Earlier than 36 Months”. He does not note in his press release “no risk for MMR and autism in everyone else”. Here is table 2 from his paper showing that.
He states a relative risk that is statistically significant for African American boys who get the vaccine before 24 months (RR=1.73) and before 36 months (RR=3.36). No increased risk for African American girls. And, as Table 3 shows, no increased risk for non African Americans.
Mr. Hooker says his results are statistically significant. Others have questioned whether his analysis is really appropriate to say this, but for now let’s just benchmark this by checking how large his sample group for that large relative risk is anyway. Just so we know. The high risk group are kids vaccinated before 36 months. Here’s a figure from Table 2 of DeStefano et al.:
There are 45 autistic kids vaccinated between 24 and 36 months. African Americans account for 40% of the total population, but let’s say about 1/2 of this 24-36 age group are African American. Or about 22 kids. 22 kids and Mr. Hooker is doing no adjustments for factors such as those found on birth certificates. The sort of socioeconomic parameters that he notes are important to get an accurate prevalence in the African American population.
Which is to say: this is not a strong finding by any stretch of the imagination.
Mr. Hooker took a subgroup–African American males–and found that there was in the unadjusted data a statistically significant relative risk. An increased relative risk is not the same thing as showing causation, especially when you are working with unadjusted data and many other limitations in this. This is enough to raise the question of whether we should do more studies to show if this increased risk holds up to further scrutiny. This is how Mr. Hooker concludes his paper:
Routine childhood vaccination is considered an important public health tool in reducing the morbidity and mortality associated with infectious diseases. However, consideration should be made in the current United States vaccination schedule for genetic subpopulations that may be associated with vaccine adverse events. Additional research is required to better understand the relationship between MMR exposure and autism in African American males.
A study relying largely on a small group of subjects (about 20) with the conclusion that more work is needed. Sounds vaguely familiar. And, as we will see, Mr. Hooker has teamed up with Andrew Wakefield to put out a video where they jump past the whole this indicates more research is needed through this is absolute evidence of MMR causing autism directly to the CDC are engaging in a racist experiment sacrificing children to autism. It’s like the events around Mr. Wakefield’s 1997 Lancet paper cranked up to 11.
Even though Mr. Hooker’s analysis is quite limited, as in it would be (and you will see is) incredibly irresponsible to jump from this to say “MMR Causes Autism in African American Males”, I’d like to see either more data or a good explanation why someone shouldn’t do it. If for nothing else, precisely to head off the sort of irresponsible and damaging PR campaign that Mr. Hooker and Mr. Wakefield have engaged in. There are a lot of data on MMR and autism since DeStefano first published (especially Hornig et al.) showing that MMR doesn’t increase autism risk. And Mr. Hooker himself has shown that autism risk is not raised in everyone other than African American boys. One can easily argue (and should) that the MMR/Autism/African American Boys result is spurious. But I’d like to see more evidence to support that. I don’t see evidence so far that this is fraud, but I don’t agree with the scientific decisions made.
All this said, can reasonable people really raise a concern about autism risk given how inflammatory that discussion can be? Yes. Here’s an example of how a study found a possible risk factor and follow up studies answered the question. The Price study was one of the largest studies on thimerosal exposure and autism risk. As part of that study they considered folic acid intake in mothers as one confounding variable for thimerosal exposure. They reported that there could be an increased autism risk from taking folic acid. The calculated risk for mothers who reported taking folic acid was about double that of those who didn’t. Keep in mind that folic acid supplementation for pregnant women is a major public health program as it reduces the risk of some developmental disabilities, so the possibility that it was increasing autism risk has major public health implications. This is a good parallel to the question of vaccines (public health program) and autism.
After the Price study, multiple studies were performed looking folic acid intake and autism risk (I can’t say that these were prompted by Price et al., but it seems reasonable to think they might):
How can we summarize the folic acid history? A possible risk factor was found. It wasn’t plausible since folic acid seems to be protective for birth defects. But people did a second check (and even a third) and found that not only is folic acid not a risk factor, it may even reduce autism risk. Which even though this is what people would have said was biologically the most probable outcome at the start, this was a needed exercise.
Can we draw a parallel? Well, DeStefano et al. and later Hooker found a possible risk for MMR and boys (with Hooker citing African American Boys) getting the MMR vaccine late but before 36 months. It doesn’t seem plausible or even self consistent with the other results of the study dataset as has already been discussed. Reasonable people could move forward on this and see if existing data could answer this or if a new study is warranted.
Reasonable people could. As I’ve alluded to, we aren’t really dealing with a “and reasonable people” scenario. And here’s where we get into the “these people are their own worst enemies” part of the discussion. We’ve already seen how Mr. Hooker has made incorrect statements about the birth certificates of the DeStefano study. Let’s look another of Mr. Hooker’s statements and ask, “is this the statement of a reasonable person”?
He added, “The exclusion is reminiscent of tactics historically used to deprive African-Americans of the vote by requiring valid birth certificates.”
And here we see Mr. Hooker and Focus Autism playing the race card for sensational effect. One can’t even say this is a stretch. It’s just ridiculous. There was no exclusion and certainly people didn’t say, “let’s exclude African Americans and deny them their rights.” Maybe some will say this still within the realm of what a reasonable person might say. I would then ask you to watch this video produced to promote this study and the events surrounding it. The really inflammatory statements are made by Andrew Wakefield, but this looks to be a joint effort between Mr. Wakefield and Mr. Hooker. If Mr. Hooker would like to explain that he disagrees with the approach Mr. Wakefield took, I’ll be quick to rewrite this. But for now, here’s what team Wakefield/Hooker has prepared for you:
As promised above here are Andrew Wakefield and Brian Hooker claiming that the CDC are running a Tuskegee like experiment, where in Mr. Wakefield’s view African American boys are allowed become autistic by MMR for some nefarious and unexplained reason (because there are so few autistics that we need to create some for study?). I suspect Mr. Hooker will take offense at me stating that he is claiming this as it’s Mr. Wakefield who says the words. OK. Go ahead and put out a statement distancing yourself from this irresponsible attack Mr. Hooker. And, yes, I wasn’t exaggerating when I said that Mr. Wakefield thinks that the CDC are even worse than Hitler, Stalin and Pol Pot. The dictators, you see, were sincere. (8:40 into the video).
No one has yet responded in the mainstream media to the press releases and the Hooker study. And many of Mr. Wakefield’s supporters online are noticing this and asking why. Here are some possibilities:
2) perhaps the most famous person in that bad science and unethical behavior is your spokesperson on this new media campaign: Andrew Wakefield.
3) members of the press are not generally attracted to stories where people who have devoted their lives to preventing infectious diseases and to understanding developmental disability are called worse than Hitler.
4) after years of a campaign to instill fear about vaccines, we are in the midst of outbreaks of multiple vaccine preventable diseases. The founder of the blog where Mr. Hooker chose to release and discuss his new results famously once bragged that his groups was going to bring the “U.S. vaccine program to its knees”
Mr. Wakefield and Mr. Hooker probably (and some of their followers certainly) have been wondering why their news of a CDC “informant” hasn’t garnered media attention. If you read the press releases and have followed the online discussions, you know that the idea for this reanalysis of the DeStefano data came from documents obtained by Congressman Issa and from phone conversations Mr. Hooker had with a CDC epidemiologist.
In their first press release, Mr. Hooker’s team noted that
According to Dr. Hooker, the CDC whistleblower informant — who wishes to remain anonymous — guided him to evidence that a statistically significant relationship between the age the MMR vaccine was first given and autism incidence in African-American boys was hidden by CDC researchers.
That was released on a Tuesday. The video came out the Monday previous, but was censored and the voice of the “informant” was obscured. On that same Monday, Mr. Wakefield noted on his Facebook page “He will be identified very soon” (referring to the “informant”). In other words, they had no intention of keeping this man’s identity secret. And a few days late, on Thursday night, the video was changed so that the censoring was gone and the voice was not obscured.
So, we have an informant who was obviously working with the Hooker/Wakefield team for months who wanted to remain anonymous. The Wakefield/Hooker team left clues about who this person was: they noted that he works for the CDC and has for some number of years and Mr. Hooker spoke of the informant as “him”. There are only two males who worked on that paper: W.W. Anderson Thompson (who has been named as the informant) and a statistician in the acknowledgments. Which of those two are on record within CDC as having voiced a strong opinion about the African American boy data? Heck, I nearly called Mr. Thompson myself to ask if he was working with Mr. Hooker. I wouldn’t be surprised if people at the CDC figured it out and that’s why his name was so quickly divulged by Mr. Wakefield. Why keep his name secret if you’ve already given out enough information to his superiors for them to break his cover?
And with that let’s get back to the “these guys are their own worst enemies” discussion. When you have someone you consider a whistleblower, it is your duty to protect that person. Not out him/her. Mr. Wakefield doesn’t seem to understand that. Years after having ignored the information given to him by a whistleblower in the UK, Mr. Wakefield not only outed that whistleblower, he first threatened the man with disclosure:
If Mr. Thompson intended to stay anonymous, and I have no reason to suspect otherwise, he chose poorly in his confidants.
Mr. Thompson had many options of to whom he could reveal his information. Many people would have taken him seriously and not taken the highly irresponsible approach that Brian Hooker has with the race-baiting video and more. I’ve read a number of people speculate that Mr. Thompson didn’t know what he was getting himself in to. If he really chose to work closely with Mr. Hooker, I can’t see how he didn’t see the extremes this information would be put to.
Mr. Hooker has had much communication with the CDC over the past decade and more. Here is some of that communication (about 3MB worth), selected by Mr. Hooker himself as an exhibit in his FOIA case with the CDC.
People at the CDC, likely Mr. Thompson included, would know of Mr. Hooker’s very strong opinions of them. A letter sent to then CDC Director Julie Gerberding is entitled “War Crimes in Your Fight Against Infectious Disease and recommends: “I would personally urge you to review the Book of Matthew 18:6 and consider your own responsibility to all children of the U.S. including my own son.” Italics in the original. Here is one version of Matthew 18:6:
But whoso shall offend one of these little ones which believe in me, it were better for him that a millstone were hanged about his neck, and that he were drowned in the depth of the sea.
Brian Hooker and Andrew Wakefield present at parent conventions such as AutismOne, where other presenters are selling their goods and services with faux autism treatments. Treatments such as bleach enemas and drinks (MMS), Lupron (a drug which shuts down sex hormone production. Essentially chemical castration), chelation, megadoses of “supplements” and more. They are sold largely on the promise of healing “vaccine injury”. By handing the Hooker/Wakefield team this PR win, Mr. Thompson will be feeding that industry.
This all said, we only have a few sentences on a video purporting to be Mr. Thompson. I have no reason yet to doubt that his his voice. I also don’t have the full conversations in context. Nor do I have evidence that Mr. Thompson agreed to be outed. Nor do I have evidence that Mr. Thompson agreed to have his phone conversations recorded. Nor do I have evidence that Mr. Thompson continues to communicate with Mr. Hooker. In fact he’s been silent since this story broke and no new quotes from him have been passed by Mr. Hooker or Mr. Wakefield.
What’s more, and rather odd, is that MMR is not really either Mr. Thompson nor Mr. Hooker’s primary interest. Mr. Thompson was author on a number of major thimerosal papers. First author on one. Mr. Hooker’s primary focus on the vaccine/autism discussion has been on thimerosal. I have been reading people online claiming that these events are what they’ve expected and hoped for: someone from CDC exposing that all the vaccine/autism work is fraudulent. But this isn’t the case at all. Nothing so far on thimerosal. One re-analysis of some MMR work that, while important to discuss, is not very strong at all. And while I have written what is possibly my longest article yet (out of something like 2000), there isn’t, as they say, much there there when it comes to anything substantial about vaccines and autism. What we do have is a public relations mess. A story that will be exploited by unethical people to frighten parents and try to revamp their own image and take some revenge.
More recently, at least one (non reliable) site is reporting that Mr. Thompson has spoken through his attorney. The message (and I paraphrase): in getting the preliminary result on African American boys out, he did what he set out to do.
In the end, it is once again public health and autism families that will pay the price. People will use this in their attempt to “bring the U.S. vaccine program to it’s knees”. More autism parents will be dragged into the self blame and guilt that comes with the vaccines-cause-autism beliefs. And disabled children will be subjected to abusive faux therapies in attempts to heal their “vaccine injury”.
A study comparing vaccinated and unvaccinated children is expected to be published soon. That study was mentioned at a meeting of the Interagency Autism Coordinating Commitee earlier this year. With that announcement one might reasonably expect much discussion in the online autism parent community. Instead I’ve seen only one response: SafeMinds (an organization focused on the failed idea that mercury in vaccines caused the rise in autism diagnoses) put an article on their website noting that they were “worried” by this study (a response I already discussed). Perhaps I missed it, but I did not see a statement in the SafeMinds article that they have their own vaccinated/unvaccinated study ongoing. Not only a vaccinated/unvaccinated study, but one which parallels the one about to be published. Both the about to be published study and the SafeMinds funded study focus on baby siblings of autistic kids. Parents of autistic children are more likely to delay or forgo vaccines than are other parents. Also, the risk of autism is high in the baby sibling population, giving a ” ‘window of opportunity’ to observe any potential interactions between vaccinations and the diagnosis of ASD”, as SafeMinds put it. But read for yourself. Under “Recently Funded SafeMinds Investigations“, SafeMinds lists:
The Early Identification of Infants and Toddlers at Risk for Autism Spectrum Disorders, Developmental Delay and Developmental Language Disorders
CAROLE SAMANGO SPROUSE, ED.D., THE FOCUS FOUNDATION
The siblings of children with Autism Spectrum Disorder have a 90% incidence of speech and language delay and an 11% increased risk for Autism Spectrum Disorder (ASD). This proposal hypothesizes that the siblings who are not vaccinated will have a smaller incidence of ASD than the 11% already projected, as well as other developmental differences. The incidence of ASD in siblings will be lower in the unvaccinated population than vaccinated. The siblings of children with ASD provide a fertile ground to follow the neurodevelopmental progression of an at-risk population, and the effects of vaccinations on development. The siblings also provide a “window of opportunity” to observe any potential interactions between vaccinations and the diagnosis of ASD. It is very common for parents of children ASD to avoid vaccinating siblings in the first five years of life. This provides an interesting opportunity to observe and see possible correlations between vaccinations and ASD.
First, let me note the wording of that webpage: “Recently Funded SafeMinds Investigations”. Not Investigations Recently Funded by SafeMinds. Their choice of word order is poor. It implies that these are “SafeMinds Investigations” and not really independent. I will note that SafeMinds were more careful at the top of that page in how they framed the projects they have funded, but still, I would change the “SafeMinds Investigations” if I were they.
When I searched for information on the principle investigator for the SafeMinds study, I found a 2007 announcement for the study: Vaccinated/Unvaccinated Autism Baby Sibling Study, Carole Samango Sprouse, Ed.D., The Focus Foundation. Research does take time, something I wish SafeMinds made more clear in their public statements. It’s been seven years, though, and I haven’t seen this vaccinated/unvaccinated study published. The only payment I’ve seen in the SafeMinds tax forms to support this project was relatively small, $24,250 in 2006, so perhaps it wasn’t well enough supported to complete. Perhaps I missed the other support.
When we consider the question of studies comparing vaccinated/unvaccinated populations, there are at least 4 in various stages. Four. That, plus the number of statements one can find online calling for such a study and we see a very strong interest in this type of study.
Here are those four studies:
1) The self-named “National Vaccine Information Center” is funding a project at George Mason University. I believe this is being performed by a member of the NVIC.
There’s a belief I’ve seen recently online claiming that studies from Scandinavia don’t relate to the U.S. because autism is rare there (3 in 10,000) and that autism in Scandinavia is primarily “high functioning”, Asperger syndrome or the like. I won’t link to the discussions as I’ve tried to avoid using the blog to continue discussions found online elsewhere.
I don’t know where this myth originated. But here’s a recent study from Sweden and this result (1.15% autism prevalence, intellectual disability in 42.6%)
The 2007 year prevalence of ASD in all children and young people was 11.5 per 1,000 (95% confidence interval 11.2–11.8), with a co-morbid intellectual disability recorded in 42.6% (41.0–44.2) of cases. We found 96.0% (92.0–98.4) of reviewed case-notes being consistent with a diagnosis of ASD, and confirmed ASD in 85.2% (66.2–95.8) of affected twins.
Yep. Prevalence comparable to the US and with a similar level of intellectual disability.
While we are at it–the prevalence is also pretty much flat for ages 9-18 (kids born from 1989 to 1998) as well.
As noted before, thimerosal exposure from infant vaccines was low in Sweden before the 1990’s and was reduced to zero in the early 1990’s. So, for few people still clinging to the “thimerosal epidemic” idea, here’s another nail to add to that coffin.
Another recent study shows prevalence in Scandinavian countries to be between .5 and 1 per 1,000.
Boyd Haley was a professor of chemistry who was very active in the failed thimerosal-causes-autism movement. He earned extra notoriety for trying to coin the phrase “mad child disease” (yes, a variation of mad cow disease) for autistic children. He also found notoriety for marketing a synthetic chemical as a “nutritional supplement”, calling it OSR#1. Prof. Haley is certainly persistent. He’s working on a clinical trial.
How did this come to pass? Well, one of the professors in Prof. Haley’s department found that a certain compound could effectively treat mining waste, removing mercury. Given his own interests, Mr. Haley started a company with an investor with the intent to bring this chelator to the public. The chelators used in medicine today were developed for lead and have been expanded to also treat mercury. I.e. there is no mercury specific chelator and this new compound would fill that gap.
All well and good, but in his zeal to bring this product to market, Prof. Haley cut a few corners. Chelators are drugs. The compound he was working on was synthetic. But Prof. Haley chose to rush the product to market as a “nutritional supplement”. Instead of calling it a chelator, he called it OSR#1. OSR standing for “oxidative stress relief”. Mr. Haley skipped the process to prove that his drug was safe and effective. Supplements have a much lower standard for safety and efficacy testing.
The FDA was not fooled. Mr. Haley and his company were given a warning letter which pointed out that the compound is not a supplement, it is a drug:
Your firm markets OSR#l as a dietary supplement; however, this product does not meet the definition of a dietary supplement in section 201(ff) of the Act, 21 U.S.C. § 321(ff). To be a dietary supplement, a product must, among other things, “bear[ ] or contain[ ] one or more … dietary ingredients” as defined in section 201(ff)(1) of the Act, 21 U.S.C.§ 321(ff)(1). Section 201 (ff)(1) of the Act defines “dietary ingredient” as a vitamin, mineral, amino acid, herb or other botanical, or dietary substance for use by man to supplement the diet by increasing the total dietary intake, or a concentrate, metabolite, constituent, extract or combination of any dietary ingredient from the preceding categories. The only substance listed as a dietary ingredient on the labeling of OSR#1 is N1,N3-bis(2-mercaptoethyl)isophthalamide. N1,N3-bis(2mercaptoethyl) isophthalamide is not a vitamin, mineral, amino acid, herb or other botanical, or dietary substance for use by man to supplement the diet by increasing the total dietary intake. Further, N1,N3-bis(2-mercaptoethyl)isophthalamide is not a concentrate, metabolite, constituent, extract or combination of any such dietary ingredient. Thus, because OSR#1 does not bear or contain a dietary ingredient as defined in section 201(ff)(1) of the Act, this product does not qualify as a dietary supplement under section 201(ff) of the Act.
Also that the company was making claims that the drug could treat medical conditions and that the labeling was misleading in this regard. Further, that the toxicity was not adequately tested nor reported.
Your website states that” [s]ome reports of temporary diarrhea, constipation, minor headaches have been reported but these are rare and the actual causes are unknown,” as well as “OSR#1 is without detectable toxicity” and “OSR#1® … has not exhibited any detectable toxic effects even at exceptionally high exposure levels.” However, animal studies that you conducted found various side effects to be associated with OSR#1 use, including, but not limited to, soiling of the anogenital area, alopecia on the lower trunk, back and legs, a dark substance on lower trunk and anogenital area, abnormalities of the pancreas, and lymphoid hyperplasia. Based on these animal studies and side effects known to be associated with chelating products that have a similar mechanism of action to OSR#1, we believe the use of your product has the potential to cause side effects, and the before-mentioned website statements falsely assert that the product does not have the potential to cause side effects. Therefore, these statements render your product’s labeling false or misleading. As such, OSR#1 is misbranded under section 502(a) of the Act, 21 U.S.C. § 352(a).
That was in 2010. Prof. Haley and his company are now back, trying to get a clinical trial started on their compound. Essentially, they are trying to do what they should have done in the first place: get proper approval for a drug. An article in Chemical & Engineering News discusses this effort. Actually, it’s part of the cover story, “Building Pharma Molecules”
The story on Mr. Haley’s Company, CTI Science, has contracted with another company, PCI Synthesis, to manufacture the new compound.
The article is, well, a bit of a sales pitch and gets a few facts wrong. There’s a bit of spin on the FDA warning letter, for example:
“The effort to develop the compound as a mercury poisoning therapy accelerated in 2010 when the company received notification from FDA that it couldn’t market NBMI as a nutritional supplement until it underwent the full drug approval process”.
As we’ve just seen above, the compound is not a nutritional supplement at all. It needs the drug approval process because it is a drug.
The CEO of PCI is quoted as stating:
“The main starting material is cysteamine hydrochloride, which is basically an amino acid and found naturally. So it has attributes that could qualify it as a natural product.”
Which was part of the sales pitch for the OSR#1 in the old days and, again, the FDA disagreed. Just because something is synthesized from a natural product, that doesn’t make it a natural product. Otherwise there would be no synthetic products at all. Everything at some level comes from a natural product.
The article discusses how to qualify for a clinical trial the product must meet current Good Manufacturing Practices (cGMP). The article states:
The primary challenge was the removal of impurities to a level that meets cGMP standards
Think about that a moment. Apparently OSR#1 was sold with more impurities than would meet this standard–a standard for food and dietary supplements.
The article notes that, yes, this compound was sold as a product at one time
Sales to date: $1.5 million, as a nutritional supplement
$1.5M in sales. And the only reason it wasn’t higher was because the FDA stepped in. It was only out for about a year, as I recall.
In animal experiments, the amount of mercury in brain tissue was not increased, but also not decreased
So, even if you believe in the failed mercury hypothesis. What exactly were you supposed to get from this compound? I somehow doubt that even the strong believers in the mercury hypothesis think that removing mercury from, say, your liver will cure autism.
It does seem that Mr. Haley and his company are doing some of the right things now. Show that this drug is safe and effective for its intended purpose: chelation. There are some problematical statements that they may market this not as a drug but as a nutritional supplement, which is a non-starter.
There are some parents who want research on vaccines and autism. I may not agree that this is the best way to spend our limited resources, but there’s no denying that this group exists and is very vocal. One thing that surprises me is that these parents appear to be unaware of vaccine/autism research that is ongoing. Not just the studies that come out that show us over and over again that autism risk is not increased by vaccines. But other projects. Biology. Studies on regression. And more. I pointed out recently that using NIH Reporter, one can find a number of projects on autism and vaccines or autism and mercury.
But NIH is not the only Federal agency funding autism research. And there are private funders as well. As I mentioned in my previous article, another place to look for funded research projects is the IACC/OARC Autism Spectrum Disorder Research Portfolio Analysis Web Tool as this includes work the various groups represented on the IACC–both Federal and Private. Unfortunately, this tool only has 2008, 2009 and 2010 projects (had the GAO not required OARC to provide a lot of information last year, perhaps this tool would be updated by now. But such is the government.) But, even with this limitation in years, let’s see what projects come up with searches for vaccines or mercury. I’ll give the titles first, and then the abstracts for these projects below.
It’s understandable that parent advocates are not aware of these projects. I’ve written about this before (“What projects are being funded in autism research? Part 1: vaccines and GI issues”) but I think it’s safe to say that parents who believe in the vaccine/autism connection do not frequent Left Brain/Right Brain. There are places on the web that carry that message (for example, the Age of Autism blog and the sites of the organizations that sponsor it). They aren’t telling their constituencies about the ongoing research efforts. As an example, as I was finishing this article, SafeMinds came out with a letter discussing how no work is being performed on vaccines and autism.
Again, this list is only for 2008, 2009 and 2010. More recent projects from NIH were discussed here.
One hypothesis regarding the association between genetic changes, environmental factors and autism is that many mutations or polymorphisms make the organism more vulnerable to later exposure in some individuals. Called the “vulnerability phenotype”, the Noble lab hypothesizes that one potential unifying theme of the vulnerability phenotype of children with ASD is that they are more oxidized. This elevated oxidation state has been shown to be sufficient to cause dramatic changes in cellular function. In this project, Dr. Noble will test the hypotheses that genetically-based differences in oxidative status are associated with differences in vulnerability to physiological stressors in vitro and in vivo, with even greater increases in vulnerability to combinations of physiological stressors. Specifically, thimerosal and other vaccine adjuvants will be studied. The second part of the study will determine if these effects on a novel regulatory pathway called redox/Fyn/c-Cbl is a necessary mechanistic convergence for increases in vulnerability caused by a more oxidized metabolic status. These results will provide a better understanding of the biochemical effects and mechanisms of possible toxicity of vaccines and vaccine additives. What this means for people with autism: These studies will initially focus on the combination of vaccine additives, but then examine whether a background genetic vulnerability phenotype affects the response to these additives. The results would provide new targets for intervention against the adverse effects of increased oxidative status in children with autism.
The overall goal of this proposal is to address immune function in children with autism, including the response to vaccine challenge, and how that relates to behavior. Evidence suggests that autism is associated in some cases with altered immune function, but the response of the immune system in children with autism to specific immune challenges, such as vaccines, has not been investigated directly. While it has been reported that some children with autism respond poorly following vaccination with symptoms ranging from rash, diarrhea, irritability, seizures, and loss of skills, no careful, thorough approach has been undertaken to fully characterize this issue, both at the biology and behavior level. We propose to use our current CHARGE (Childhood Autism Risks from Genetics and the Environment) and Autism Phenome Project (APP) study population to address this critical issue. The overall approach would include an examination of the immune response to both viral and bacterial vaccines in children with autism, as compared to typically developing age-matched controls, in real time following vaccination at 5 years of age. Vaccines have advantages for directly studying the immune response as they provide a known, scheduled immune challenge, whose dose is well characterized – making it possible to collect and interpret immune response data at the time that it occurs. Therefore, we think that exposure to an immune challenge with vaccine would result in an increase in inflammation compared to controls in a subpopulation of children with autism. However, we also anticipate that some children will respond to vaccine challenge differently, depending on form of the vaccine, i.e. viral vs. bacterial. Thus, we propose to address the issue of immune function in children with autism through a careful analysis of the immune system, medical and mitochondrial issues, and behavioral response to both viral and bacterial vaccines.
A major challenge to studying autism with a suspected vaccine-related regression is identifying children with acute regressive-type symptoms following MMR vaccination; there are no specific codes, tests, or procedures that identify this occurrence with a high degree of specificity. This study will explore the Kaiser Permanente electronic databases to ascertain whether we can identify children with regressive type autism and identify the timing of the regression in relation to the period directly following MMR vaccination. In order to see if identification of regressive autism from medical records is possible, the investigators will attempt to identify children vaccinated with MMR who then abruptly undergo a ‘cluster’ of visits, tests, and/or procedures in the time period directly following vaccination. The researchers feel that there may be a number of children who receive a diagnosis (such as ‘prolonged crying’) in the emergency department on the day after vaccination, followed shortly thereafter (1-2 days later) by another set of diagnoses (such as ‘fever’ & ‘irritability’) in the pediatric office or other outpatient department, and then receive either diagnostic or laboratory tests indicating (at least) a moderate degree of severity of concern, such as CT scans, metabolic testing, or referral to neurology. If this study is successful in using medical databases to identify a specific group of children with demonstrable autism-related regression that clearly follows vaccination, it may point to the feasibility of further studies concentrating on this specific population.
The Thimerosal and Autism Study is a case-control study conducted in three U.S. managed care organizations (MCOs). Data collection began in 2005 and took three years to complete. In this study, children who were diagnosed with autism were matched with control children. The autism diagnosis of the case samples was confirmed by a standardized clinical assessment protocol. Vaccination histories and information on other potential confounding factors were confirmed by reviewing the medical records for all children. In addition, the mothers of both cases and matched controls were interviewed.
This project will investigate the role of three separate factors in an animal model of autism spectrum disorder: a) genetic susceptibility, b) hormonal environment, and c) possible environmental triggers. A mouse model with a mutation of the reelin gene, implicated in autism spectrum disorders, will be studied after exposure to methyl and ethyl mercury. Both behaviors and neuropathological endpoints will be explored. Finally, the role of endogenous sex hormones will be examined by eliminating the testosterone “surge” around the time of puberty. The individual effects of each will be examined, as well as the interaction of the three components (genetic liability, environmental exposure, hormonal influences) to determine gene x environment interactions. What this means for people with autism: This study will use a unique design to study multiple factors in the etiology of autism spectrum disorder in a mouse model, isolating and combining factors which previously have been implicated in the pathophysiology and behavioral phenotype.
Two independent lines of evidence indicate that the maternal immune system and a functional genetic variant contribute to autism spectrum disorder (ASD) risk. Here, the Van De Water lab will partner with scientists at Vanderbilt University to examine whether these two seemingly unrelated contributions may converge to define a unique ASD susceptibility. Preliminary evidence collected by the Van De Water lab indicates an association between the Mesenchymal epithelial transition factor (MET) gene ‘C’ type, which reduces MET protein expression, and the presence of specific maternal anti-fetal brain autoantibodies. This relationship suggests that this as a pathway for production of the maternal autoantibodies, leading to a gene x environment interaction underlying ASD susceptibility. The next line of experiments will examine the relationship in an even larger sample and assess the functional effect of the MET gene polymorphism on immune cell activity as well as further examine the impact of environmental toxins (including ethyl mercury) on the gene expression-dependent function of maternal immune cells.
The prevalence of autism spectrum disorders (ASD) appears to be on the rise in developed countries and has become a serious public health concern. In most developing countries, however, the nature and prevalence of factors associated with ASDs are unknown. The long term goal of this planning project is to develop capacity for conducting large scale population-based ASD studies in Jamaica. First, the diagnostic criteria used in Jamaica and the United States will be compared. Then, questionnaires regarding the demographic and socioeconomic position, occupation, and drinking habits of each child’s parents will be used, and information will be gathered about family history of developmental disorders, family size, birth order of the affected child, and whether the child is taking any medications. An age and sex matched case-control study, including a dietary questionnaire, will also be conducted to investigate whether environmental exposures to mercury, lead, arsenic, and cadmium play a role in autism. Blood and saliva samples will be collected to determine if any DNA polymorphisms that might affect interactions with heavy metals are present in children with ASD. New knowledge of potential environmental risk factors for ASD may arise from this research, thereby reducing physical, psychological, and economic burdens on the child, family, and society and helping parents make decisions about avoiding exposure to environmental contaminants.
An investigation into the influences of demographics and environmental variables in the development of neurodevelopmental problems such as AD, ASD, and ASD-regression
Further investigation into preliminary data that neurotensin (NT) stimulates mast cell activation and that NT is elevated in young children with autism spectrum disorder.
Autism has been associated with epigenetic changes: Tiny chemical tags in the regulatory regions of genes that affect how genes express themselves by turning them on or off. One gene often decreased in expression in the brain tissue of autistic individuals is MECP2, a gene that governs the expression of genes crucial to brain development. Exposure to environmental pollutants is also thought to play a role in autism. These two phenomena both involve a small cellular organ called mitochondria. The suspect environmental pollutants are toxic to mitochondria, which play a critical role in epigenetics: Pollution exposure can lower the amount of mitochondrial DNA (mtDNA) in a cell, causing an increase in placement of epigenetic tags by DNMT1 that leads to gene silencing. We hypothesize that exposure during pregnancy to pollutants toxic to mitochondria causes a decrease in mtDNA copy number and increased placement of epigenetic tags by DNMT1 on key developmental genes, affecting pathways that have direct roles in the development of autism. We will expose mice, during pregnancy, to selected toxicants and evaluate adult behavior and associated biochemical changes in brain tissue. Valproic acid will be used as a positive control, with saline as a negative control. The environmental pollutants lead, arsenic, cadmium, manganese, mercury, and permethrin will be investigated for their potential to induce autistic behavior changes. Brain tissue will then be used for molecular studies of mtDNA copy number, expression of DNMT1, and alterations to the epigenome on both a genomewide and gene-specific level.
—
By Matt Carey
Note: I serve as a public member to the IACC. My views here and elsewhere are my own, not those of the Committee.
This question gets brought up a lot by some parent advocates. The are informed by groups promoting the idea of vaccine causation that the government is blocking this work. The evidence points strongly away from vaccines as a primary cause of autism, and investment in this area doesn’t seem wise. At least that’s the viewpoint of the majority of parents (including myself), autistics and researchers. But some remain unconvinced and want vaccine/autism research performed. And they are upset that none of this work is being performed.
Here’s a different question: why are the groups who promote the idea that vaccines cause autism failing to inform their members that, yes, indeed vaccine/autism research is being performed?
Or, to put it simply: vaccine/autism research is being performed and it’s being funded by the government. But you wouldn’t know that if you read, say, the Age of Autism blog, Generation Rescue’s website, SafeMinds’ website, or the other groups advocating for this research. If you are interested in vaccine/autism research and you are reading about these projects for the first time here, ask yourself “why have these orgs not informed me of this?”.
As noted here recently, Tom Insel discussed an upcoming vaccine/autism study. Already commissioned, performed and in the publication stage. That announcement was in April. What was the response from the community that has pleaded for vaccine/autism research? For the first few months: Silence. In July, SafeMinds finally put out an article showing that they were “worried” about this study. I don’t see much discussion of this announcement from other groups or outlets.
I’m not surprised by this. I’ve noted before that work on areas such as vaccines, mercury, environmental risk factor research and GI dysfunction don’t get discussed by the groups that are focused on these topics. I’ve covered the research in these areas more than they have.
So let’s get back to what other work is going on in vaccines and autism. Let’s start with the simple question: how would you find out? One place is the IACC/OARC Autism Spectrum Disorder Research Portfolio Analysis Web Tool. That could use updating, but it is an easily searchable database. Another place is NIH Reporter. It’s less easy to use than the Portfolio Analysis Tool and includes all of NIH. I.e. it covers non autism topics and doesn’t include projects being done outside of NIH (say, by Autism Speaks or other private funders). But, search Reporter for autism and vaccines or mercury and what do you get? Quite a number hits. Let’s consider a few.
There are more projects. Some I left out because they are older. But I think the point is made and is very clear: vaccine/autism and mercury/autism research are being funded.
And that is without even discussing how research on the biology of autism feeds into all etiological questions. Whether it’s vaccine, genetics or what have you, if you understand the biology, you have a better chance of understanding the cause. (when I searched NIH Reporter with the terms Autism and Immune, I got 25 pages of hits. Sure, not all are on-topic, but that’s 25 pages, 606 topics).
Here are the full abstracts–with emphasis added by me–for the NIH Reporter projects mentioned above.
Abstract Text:
Reports of increasing prevalence of autism spectrum disorders (ASDs), a set of highly genetic conditions, are intensifying interest in the role of environmental exposures, including infectious, immune, and toxic factors. Retrospective studies exploring associations between environmental factors and ASDs are compromised by selection bias, small sample sizes, possibly invalid diagnosis, and absence of biologic measures. This prospective study will employ an unselected birth cohort of 75,500 in which cases are ascertained through screening of the entire population, diagnoses established using uniform procedures, extensive histories and clinical data obtained, and biologic samples collected serially throughout pregnancy and early childhood. The application of high throughput laboratory assays to derive maximal information from developmentally-influenced, finite, and nonrenewable biologic samples, and inclusion of early screening and diagnostic assessments, will permit an unprecedented, rich view of the longitudinal trajectory and nascent signs and symptoms of ASDs, facilitate discovery of biomarkers, and afford unique insights into the role of gene:environment interactions in ASD pathogenesis. Specific aims are to: (1) establish the autism Birth Cohort (ABC) through ascertainment of cases of autism spectrum disorder (ASD, N=150-233) and selection of controls (N-1000) from the Norway Mothers and Child (MoBa) cohort; (2) examine biologic pathways that may predispose to ASD, through evaluation of immune, endocrine, and neuroregulatory factors in mothers during early gestation or at birth and in children, at birth or 30 months postnatal; (3) identify environmental factors that may be directly or indirectly associated with ASD, including pre- or postnatal infection, vaccination, very low birth weight or other obstetric risk factors in which infections are implicated, dietary and/or environmental exposure to methylmercury; (4) describe the natural history of clinical, anthropometric, and neurobehavioral features of ASD; and (5) explore genotypic influences that may be directly or indirectly associated with ASD by testing associations of ASD and/or its endophenotypes with family history of autoimmune disease or selected candidate genes, and investigating conditional gene-environment effects using antecedent factors found to influence ASD risk.
Abstract Text:
This subproject is one of many research subprojects utilizing the resources provided by a Center grant funded by NIH/NCRR. Primary support for the subproject and the subproject’s principal investigator may have been provided by other sources, including other NIH sources. The Total Cost listed for the subproject likely represents the estimated amount of Center infrastructure utilized by the subproject, not direct funding provided by the NCRR grant to the subproject or subproject staff. Diagnoses of childhood developmental disorders involving autism-spectrum symptoms are increasing, estimated to affect 1 in 100 children in the United States. Childhood Vaccines have been hypothesized to be contributory factors to this increase. The childhood vaccine regimen has an experimentally unstudied potential for cumulative and synergistic toxicities and possible immunologic interference to normal development. A prior study developed a primate model to assess neurodevelopmental consequences of the 1994-1999 pediatric thimerosal vaccine regimen (1994-1999). Significant neurodevelopmental deficits were evident for vaccinated animals in survival reflexes and standardized cognitive tests, and exposed animals developed gastrointestinal inflammation associated with focal transmural colitis, lymphoid hyperplasia, and syncytia.
Abstract Text:
The long range goal is to determine if exposure to environmental toxicants early in development contributes to the etiology of neurodevelopmental disorders such as autism. A related goal is to determine whether susceptibility to autoimmune disease increases the neurotoxicity of environmental contaminants and increases the risk for developing disorders such as autism. Understanding how exposure to environmental toxicants may contribute to the etiology of neurodevelopmental disorders is important so that the exposure risks can be identified and minimized. If immune system dysfunction is found to increase the risk of exposure to environmental toxicants, then exposure limits to toxic substances can be lowered, and children with immune system dysfunction who may be at increase risk can be identified and protected. The specific aims are to expose mouse strains with low (C57BL/6J) or high (SJL mice) susceptibility to autoimmunity perinatally to either methylmercury (MeHg), polychlorinated biphenyl 95 (PCB 95) or polybrominated diphenyl ether 47 (BDE 47). We will then compare the effects of toxicant exposure between these mouse strains on brain development, complex social behaviors, and immune system function. The hypothesis is that perinatal exposure to each of these toxic substances will impair brain development and behavior, and that suscepbility to autoimmune disease will increase the neuro- and immunotoxicity of these agents. We will also explore a potentially new model of autism in mice injected prenatally with unique autoantibodies isolated from the serum of mothers who have given birth to two more more autistic children. Brain development will be examined histologically using stereological procedures and immunohistochemistry. Complex social behaviors will be studied using behavioral testing procedures established in our laboratory that measure social recognition, social interaction and social communication in mice. Immune system status will be established by measuring cytokines, chemokines, immunoglobulins, and quantifying immune system response to antigenic stimulation. In addition, seizure susceptibility will be measured in toxicant-exposed mice as well as measures of synaptic excitibility and plasticity in hippocampal brain slices. These studies will provide critical new information on the role of the immune system and its interaction with environmental contaminants in autism and other neurodevelopmental disorders.
NIH Spending Category:
autism; Autoimmune Disease; Behavioral and Social Science; Brain Disorders; Epilepsy; Mental Health; Mental Retardation (Intellectual and Developmental Disabilities (IDD)); Neurodegenerative; Neurosciences; Pediatric; Perinatal Period – Conditions Originating in Perinatal Period
IMMUNOLOGICAL SUSCEPTIBILITY OF AUTISM. Abstract Text:
Recent studies indicate that immune function in children with autism spectrum disorder (ASD) is profoundly altered compared to developmentally healthy controls. There is a strong interface between the immune system and the neurologic network, and successful neurodevelopment is contingent upon a successful interaction between these two systems. We have identified several aspects of immune dysfunction in patients with autism compared with typically developing controls. These include a reduced response to vaccine antigens of bacterial origin, altered cytokine levels in plasma and upon stimulation of PBMC, increased levels of leptin in patients with early onset autism, and autoantibodies to brain antigens. This wide and complex variety of immune anomalies noted in our first funding period is in keeping with the broad range of phenotypes encompassed by the autism spectrum. Thus, we will build upon our earlier findings of both serologic and cellular changes in immune function. While our studies in the previous project period were aimed at a broad analysis of immune function in patients with autism, the current proposal will address the mechanisms responsible for the numerous alterations in immune homeostasis uncovered in our earlier studies. Therefore, our primary focus will be on the mechanisms responsible for such anomalies in immune function through an in depth analysis of cellular immune function. Our overall hypothesis is that patients with autism have a fundamental defect at the cellular level that ultimately leads to abnormalities in immune function and heightened susceptibility to environmental triggers. To examine this, we propose to: (1) examine longitudinally the serologic profile of children with ASD to ascertain whether the various immune changes noted in our first studies are maintained and/or deteriorating further; (2) determine which immune cell population(s) plays a critical role in the immune dysfunction seen in patients with autism; and (3) fully characterize the autoantibody response in a subpopulation of children with ASD and some mothers of children with ASD. It must be noted that due to the highly heterogeneous nature of autism, there will potentially be immunologic differences that relate to sub-groups of patients with autism. Therefore, we will carefully define the study groups based on our current data to include children with early onset autism, children with delayed onset/regressive autism, general population controls, and children with developmental disorders without ASD. The studies will be performed on CHARGE subjects formerly analyzed by our laboratory (CHARGE-BACK study). This will allow us to extend our prior studies longitudinally to determine if the immune dysregulation, such as increased leptin levels in the early onset patients, remains over time. The following aims address both the serologic and cellular aspects of immune function in patients with autism.
Abstract Text:
This contract modification is to extend and supplement Contract HHSN271201000033C, consistent with the scope of work of “Study of Health Outcomes in Children with autism and Their Families¿ in order to access the currently validated database developed under the contract to provide for further analysis . Autism Spectrum Disorder (ASD) is a significant public health concern, with an estimated prevalence of 1 in 88 children in the United States. Much of the research to date has focused on the core social and communication deficits of ASD, but there are anecdotes and some survey data suggesting that the rate of comorbid health conditions may also be elevated in this population. Furthermore, despite several large-scale epidemiological studies that have assessed but not found any potential association between ASD and vaccinations, public concerns persist about such a causal link. At least partly as a consequence, health officials in the United States have reported an increased rate of vaccine refusal in the general population. The Study of Health Outcomes in Children with autism and their Families was begun two years ago. Under this contract, the Contractor analyzed a large dataset of retrospective commercial health plan claims of 46,236 children with ASD, their parents and siblings, and a comparison cohort of children and family members. They successfully completed the analyses requested in the original statement of work, which included a study of the validity of ASD diagnoses in the claims data, and descriptions of health outcomes and health care utilization of the ASD cohort, their family members, and the comparison cohorts.
NIH Spending Category:
autism; Brain Disorders; Immunization; Intellectual and Developmental Disabilities (IDD); Mental Health; Pediatric; Prevention; vaccine Related
Project Terms:
Anecdotes; autism spectrum disorder; Autistic Disorder; Child; cohort; Contractor; Contracts; Data; Data Set; Databases; Diagnosis; Epidemiologic Studies; Family; Family member; General Population; Health; health care service utilization; Health Planning; Link; Modification; Outcome; Parents; Population; Prevalence; public health medicine (field); Recording of previous events; Reporting; Research; Siblings; social communication; Surveys; United States; Vaccination; Vaccines; Work
Core 4 is the Molecular Core. It serves as the central resource for the projects that isolate and process RNA on Affymetrix microarrays, and for performing RT-PCR confirmation of the microarray data for those projects. The UCD Affymetrix Core Facility is run by Dr. Jeffrey Gregg and is equipped with fluidics stations, hybridization ovens, and the new scanner required to scan the human Affymetrix U133 2.0PLUS arrays. Preliminary data from the previous CHARGE study has shown that there are changes in gene expression in the blood of children with autism compared to control children in the general population (GP) and to control children with mental retardation and developmental delay (MR/DD). The blood genomic profile in children with autism without regression (A) was different from controls, autism spectrum disorder (ASD) and different from children with autism with regression (A-R). In addition, there is a group of regulated genes in most children with A, A-R and with ASD that are expressed by natural killer (NK) cells in peripheral blood, suggesting an abnormality in this cell type that is common to all types of autism. These NK-cell related genes are expressed by all of the autism phenotypes including A, A-R and ASD, and hence may point to common pathways that underlie the common language and behavioral abnormalities in all three disorders. This core will be utilized by the projects as follows. Project #1: Aim #1: Perform genomic (RNA expression on microarrays) studies on blood from children with autism in the 4-9 year old range, and compare to the blood genomic profiles we have obtained in children with autism in the 2-5 year old age range. Aim #2. Compare gene expression as a function of blood metal levels in both age groups in A, A-R, ASD, MR/DD and GP groups. Aim #3. Examine genomic profiles in pregnant mothers who have previously given birth to an autistic child to determine if there is a specific genomic profile that correlates with whether the mother’s fetus is destined to develop autism. Project #2. Aim #1. Describe the gene expression profiles in the blood using specific white blood cell subsets including NK cells for children with autism without regression, autism with regression, and ASD children compared to GP and delayed children. Aim #2. Examine gene expression following stimulation or activation of specific white blood cell subsets of A, A-R, ASD, MR/DD and GP children with: low level mercury; immune cell stimulation/activation with vaccine antigens and cell-specific mitogens; and xenobiotics. Project #3. Compare gene expression profiles in the blood of children with autism to the blood of experimental animals exposed to toxicants including organic mercury, PCB 95, and PBDE 47 (Project #3).
Abstract Text:
DESCRIPTION (provided by applicant): Few rigorous epidemiologic studies have addressed the environmental causes and biologic underpinnings of autism spectrum disorder (ASD). The CHARGE (Childhood autism Risks from Genetics and Environment) Study is a large, population-based case-control investigation of environmental risk factors, broadly defined, in relation to ASD and developmental delay without ASD symptoms, with referents from the general population. Fieldwork began in 2003, and by now CHARGE has published widely on exposures such as air pollution, mercury, flame retardants, maternal nutritional status in the peri-conception, untreated fever during pregnancy, mitochondrial dysfunction, candidate genes, a wide array of functional immune markers in both the child and the mother, and maternal metabolic conditions including obesity and diabetes. This last finding is notable, given the epidemic of obesity and type 2 diabetes that has occurred in parallel with the steady rise in ASD over the last few decades. Moreover, an emerging literature implicates several endocrine disrupting chemicals as contributing to obesity and metabolic dysregulation, including hyperinsulinemia, and to neurodevelopmental disorders as well. This project therefore builds upon these observations in several ways. First, obesity and type 2 or gestational diabetes will be examined in a larger sample, and glucose challenge test (GCT) results for the first time, to determine associations not only with development of ASD and intellectual impairment in the children, but also with specific speech and language delays, behavioral phenotypes such as attention deficits or hyperactivity, and gene expression. Second, these maternal metabolic conditions will be evaluated for associations with markers of both metabolic and immune dysregulation to be measured in neonatal bloodspots. Third, the predictive value of neonatal bloodspot markers for a later diagnosis of ASD or other child developmental and behavioral outcomes will be assessed. Fourth, the maternal metabolic conditions will be analyzed for potential links with upstream exposures to phthalates and anti- bacterial compounds, ubiquitous chemicals in common household products. Finally, this project will examine how gene variants that play a role in biochemical pathways relevant to the processes under study may influence susceptibility of the mother, the neonate or the child. To ensure adequate power for this analysis of gene-environment interaction, the sample size will be increased to 2400 children. This project addresses several goals set by the NIH Interagency autism Coordinating Committee: 1) to discover environmental factors contributing to ASD, particularly in the prenatal period, 2) to understand biological mechanisms for ASD risk, including gene-by-environment interactions, and 3) to identify children at risk for ASD at earlier time points. Results of this detailed inquir into early exposures, maternal pathophysiology and prognostic markers in the newborn will set the stage for developing prevention strategies.
Public Health Relevance Statement:
PUBLIC HEALTH RELEVANCE: This project addresses several issues of direct public health relevance, and the science to be produced will lead to benefits in a wide cross-section of the U.S. population. Because obesity is reaching epidemic proportions and other metabolic conditions such as Type 2 diabetes, gestational diabetes, and dyslipidemia are rising steeply, understanding environmental causes has tremendous public health potential for moving us closer to effective prevention strategies. If environmental chemicals used in common household products do prove to adversely affect body weight, measures can be taken to either reformulate those products, removing them from the market, or to educate consumers on how to avoid them. Similarly, steady increases in ASD might be curbed if the postulated causal pathway is supported by the evidence.
NIH Spending Category:
autism; Behavioral and Social Science; Brain Disorders; Clinical Research; Diabetes; Genetic Testing; Genetics; Intellectual and Developmental Disabilities (IDD); Mental Health; Neurosciences; Nutrition; Obesity; Pediatric; Perinatal Period – Conditions Originating in Perinatal Period; Prevention
DESCRIPTION (provided by applicant): Little is known about the etiology or risk factors for autism, a disease affecting 1 in 50 children in the U.S. While genetic and environmental factors are thought to act together, the specific mechanisms are not known and the measurement of environmental risk factors during critical periods of neurodevelopment has been lacking. This case-control study seeks to apply a novel dental biomarker of early life metal exposure, including in utero, to identify risk factors for ASD. Beyond looking at exposure intensity, we will be able to identify differences in exposure timing between cases and controls. This will allow us to identify critical windows when exposure, even at low levels, increases the risk of ASD. Using the proposed biomarker, we will directly assess fetal exposure, and will not rely on maternal biomarkers which may only provide an indirect measure of fetal exposure to metals. This work will have substantial impact on epidemiologic investigations of the relation of early life chemical exposures to ASD and other neurodevelopmental disorders as it can be used to objectively reconstruct both exposure intensity and timing.
Public Health Relevance Statement:
PUBLIC HEALTH RELEVANCE: Little is known about the causes of autism. This proposal seeks to apply a novel dental biomarker of early life metal exposure, including in utero, to identify risk factors for ASD. Beyond looking at exposure intensity, our application is novel in that we will be able to identify differences in exposure timing between cases and controls. This will allow us to identify critical windows when exposure, even at low levels, increases the risk of ASD.
Autism in the U.S. Somali Community has gathered significant attention in recent years (as has autism in other Somali communities outside of Somalia, for example in Sweden). Most of the attention in the U.S. can be traced back to vigorous advocacy by people like my fellow IACC public member Idil Abdul. Not all attention is good. For example, Minnesota Somali parents received a lot of attention from groups promoting the failed vaccine/autism link. When news of the possibly high prevalence in the Minnesota Somali community arose, David Kirby used the story to promote the idea of vaccines causing autism. Generation Rescue brought in Andrew Wakefield to talk to Somali parents in closed door meetings.
There are limitations to the study, such as the use of a “convenience sample” of parents attending one specific clinic. This could induce bias. Also, the response rate was about 50%. This is reasonable, but again some bias might be involved in who actually responded. People who distrust vaccines might distrust those performing the survey, for example.
To answer the question–yes, Somalis in Minnesota do think that the MMR causes autism more than their non-Somali counterparts. Nearly 5 times more likely. But, the majority do not believe–about 35% of Somali parents and 8% of non-Somali parents believe that autism is caused by vaccines.
At recent IACC meetings, Idil Abdul has related how she knows Minnesota Somali families who stopped vaccinating after having a first autistic child. These families went on to have more autistic children. Unvaccinated autistic children. In one family, she relates a family with 5 autistic children.
This stands as an example of where we in the autism parent community have failed. We scared the parents in the Minnesota Somali community, sending in Generation Rescue, Andrew Wakefield and David Kirby. Parents stopped vaccinating, offering zero protection from autism but leaving their children open to infectious diseases. To say nothing of the guilt that parents feel and the children who grow up under that falsely placed guilt.
Yes, I stand apart from the minority of parents spreading the message of a vaccine-epidemic. But, as a community, we have to accept our failures as a community. And this is an example of a big failure.
Here is the abstract.
Abstract
BACKGROUND:
In 2011, an outbreak of measles in Minnesota was traced back to an unvaccinated Somali child. The purpose of this project was to (1) ascertain whether Somali parents are more likely than non-Somalis to refuse childhood vaccinations, particularly the measles-mumps-rubella (MMR) vaccine and (2) determine what factors influence the decision not to vaccinate.
METHODS:
We explored parental perceptions and utilization of vaccines through a survey distributed to a convenience sample of Somali and non-Somali parents of children ≤5 years old in a family medicine clinic in Minneapolis, MN.
RESULTS:
A total of 99 surveys were completed, 28% (n = 27) by Somali parents. Somali parents were more likely than non-Somali parents to have refused the MMR vaccine for their child (odds ratio, 4.6; 95% confidence interval, 1.2-18.0). Most of them refused vaccines because they had heard of adverse effects associated with the vaccine or personally knew someone who suffered an adverse effect. Somali parents were significantly more likely to believe that autism is caused by vaccines (35% vs. 8% of non-Somali parents). Somalis were also more likely to be uncomfortable with administering multiple vaccines at one visit (odds ratio, 4.0; 95% confidence interval, 1.4-11.9) and more likely to believe that children receive too many vaccines.
CONCLUSIONS:
Statistically significant differences in perceptions and use of vaccines were reported by Somali and non-Somali participants. Somali parents are more likely to believe that the MMR vaccine causes autism and more likely to refuse the MMR vaccine than non-Somali parents. These beliefs have contributed to an immunization gap between Somaliand non-Somali children
What did they find? That parents often delayed vaccines for younger siblings of autistic kids. And that this made no difference on the autism rate in those younger siblings. In fact, most of the younger siblings with ASD diagnoses were not fully immunized.
This isn’t a study of just MMR or just thimerosal. It’s all vaccines. In online autism/vaccine discussions, you will often read something to the effect of “only one vaccine and one ingredient have been studied”. Wasn’t true before this new study. Isn’t true now. Will be even less true when the next study comes out.
Why do I suspect that “Dr. Bob” Sears, SafeMinds, Generation Rescue, the National Autism Society and TACA won’t include this study in the literature they bring to parents’ attention?
Background: Parental concerns persist that immunization increases the risk of autism spectrum disorder, resulting in the potential for reduced uptake by parents of younger siblings of children with autism spectrum disorder (“younger sibs”). Objective: To compare immunization uptake by parents for their younger child relative to their older child with autism spectrum disorder (“proband”) and controls.
Design: Immunization status was obtained for 98 “younger sibs,” 98 “probands,” and 65 controls.
Results: A significant group difference emerged for overall immunization status (Fisher’s exact test = 62.70, p < .001). One or more immunizations in 59/98 younger sibs were delayed (47/98; 48%) or declined (12/98; 12.2%); immunizations were delayed in 16/98 probands (16.3%) and declined in only one. All controls were fully immunized, with only 6 (9.2%) delayed. Within the "younger sibs" group, 25/98 received an autism spectrum disorder diagnosis; 7 of whom (28%) were fully immunized. The rates of autism spectrum disorder diagnosis did not differ between immunized and nonimmunized younger sib groups, although small sample size limits interpretability of this result.
Conclusion: Parents who already have one child with autism spectrum disorder may delay or decline immunization for their younger children, potentially placing them at increased risk of preventable infectious diseases.
Yes, this is a different topic than typical for this blog. But, let’s consider a simple and obvious lie by our president: the As is typical for this president, this project involves multiple lies. Here are but two. First, the White House would not be changed itself. Just added to. As noted in a recent […]
How does one recapture trust in the public health system? I can tell you one way to make it worse. Put Mark Baxill to work at the CDC. Mr. Blaxill is a long time anti-vaccine activist who has done a lot of harm promoting the “vaccines cause autism” lie. We on this blog have been […]
The same people who might value your efforts with Operation Warp Speed will also be able to do the simple math in their heads that says Mr. Kennedy’s approach is going to kill people. Mr. Trump, there is a lot of chatter about you wanting the Nobel Peace Prize. OK, I know you’ve publicly stated […]
We pay for the CDC. It isn’t there to support Mr. Kennedy’s agenda. It’s there to generate good information that Mr. Kennedy can use or, sadly, not use. He can’t ask them to sign off on dangerous vaccine policy and then cry “restore trust” to excuse firing the trusted experts who are, in his own […]
I will state this straight out–I believe the anti vaccine movement has put good people at risk for decades with their rhetoric. And I also believe Mr. Kennedy has contributed a great deal to this climate of hate. How much or how directly he may have influenced the gunman who opened fire at the CDC […]

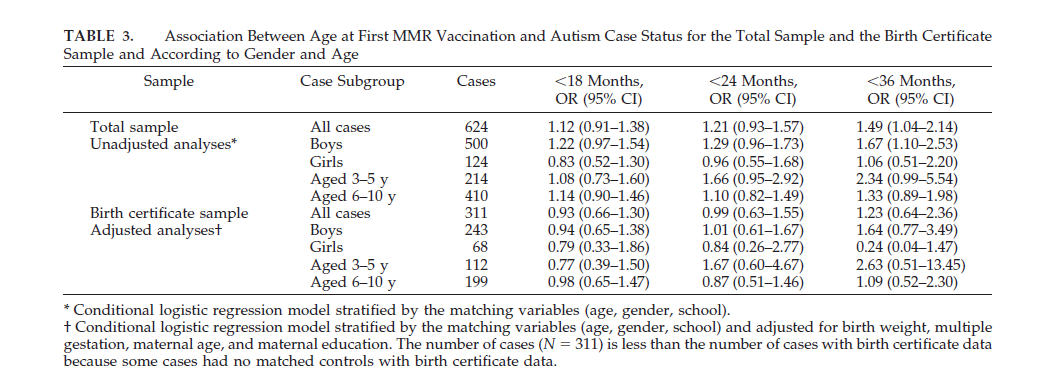
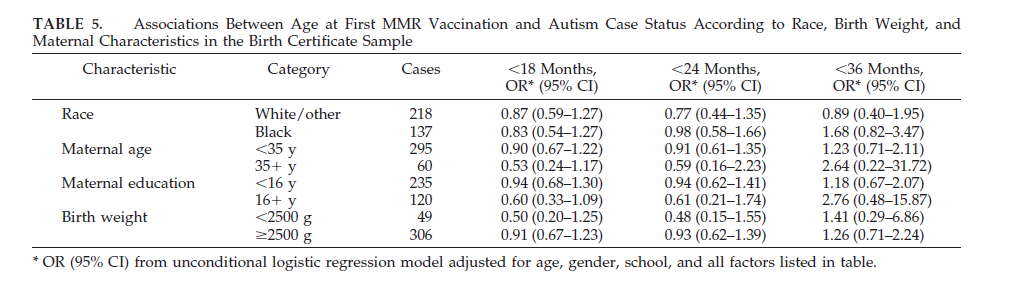
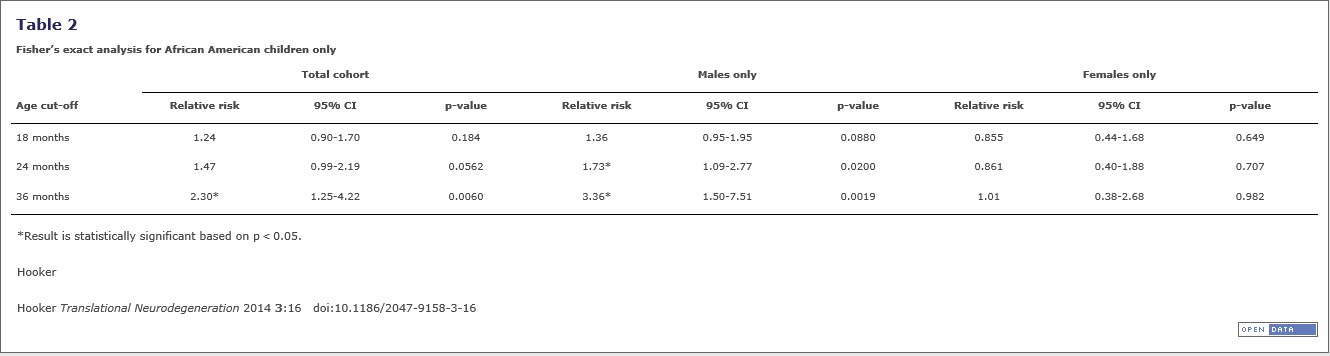
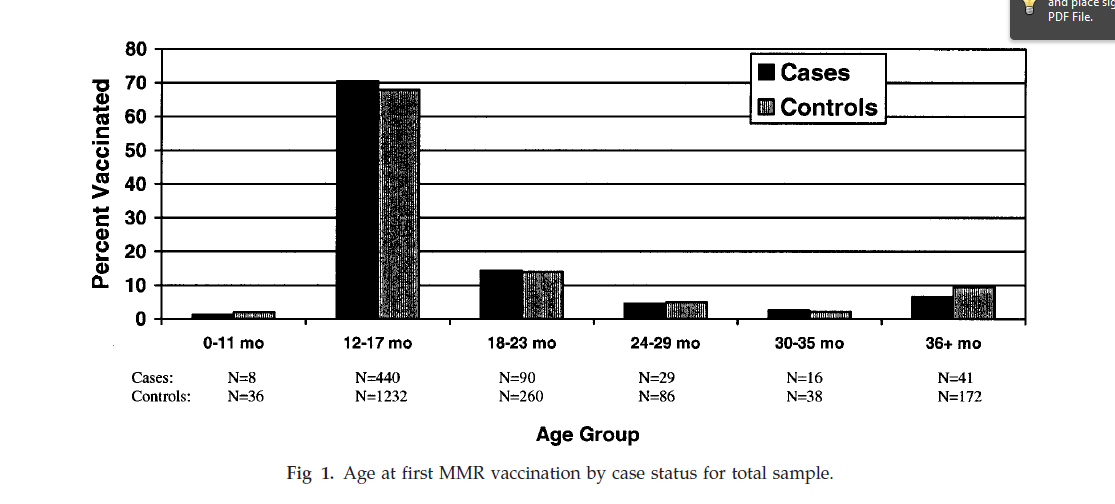
![plos_sweden_figure_1_top[1]](https://leftbrainrightbrain.co.uk/wp-content/uploads/2014/07/plos_sweden_figure_1_top1.png)
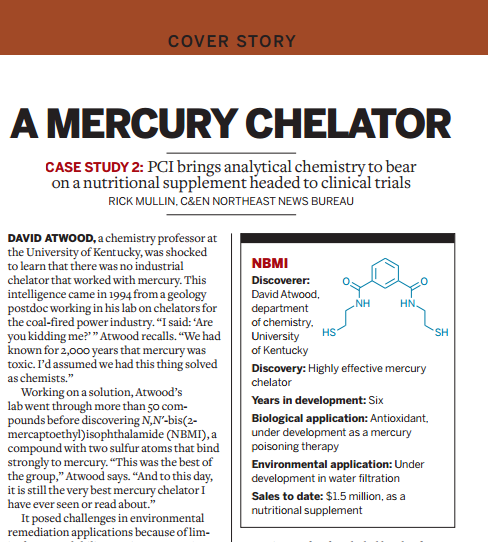

Recent Comments