The CDC came out with a new autism prevalence estimate yesterday. Their estimated autism prevalence is 1.68%. That’s up from the estimate from 2 years ago (1.46%), but lower than a different recent study (2.76%).
I’m going to discuss some minor-league shenanigans. It’s no surprise that some groups abuse facts and cherry pick data to make political points. In this case it was useless. there was no need to cherry pick. I’ve done a lot of exposing the abuse of facts by some so-called autism advocacy groups. I don’t get any joy from noting that people in my community are both dishonest and ignorant of science. But much as that bothers me, it pales in comparison to the lost opportunities. Millions of dollars were spent on this prevalence estimate alone, but all some groups do is dig for reasons to justify their “epidemic” story and push the long-ago failed idea that vaccines are to blame.
Over the years, news organizations and autism groups have jumped at the chance to put their spin on each new CDC autism prevalence estimate. Over the years I’ve spent a lot of time trying to unspin the takes of groups like the Age of Autism blog. AoA is, well…if you want to see autism done wrong, read the Age of Autism blog. Science, medicine, human rights and dignity, they can be counted upon to get things wrong.
With that in mind I decided the CDC announcement was a time to break my current trend of ignoring AoA. I literally haven’t read it in months. What I saw was both surprising and typical for them. Surprising in that they didn’t even bother to write their own pieces for the new prevalence numbers. Seriously–they just copied a couple of articles from other sites and left it at that.
By the way–this new low-level interest in autism prevalence appears to me to be a general trend–beyond just AoA. Autism is losing it’s status as having intense focus from the US media and public. The chance to leverage the public’s interest into meaningul change is waning. That’s a far more interesting topic and far more important than this and I want to come back to it in the future.
So, what did AoA post? Big League Politics BREAKING: CDC Reports 20 Percent Autism Increase In Children and Breaking News: 1 in 59 children Born in 2006 have Autism, 1 in 36 between the ages of 3 and 17. What’s going on?. That first one caught my eye. First because in absolute terms, the autism prevalence increased by 0.22%. In relative terms, that’s about a 15% increase. They could have said 15% and made their point, but why do that when 20% is even more scary? More to the point–digging just a little into this 20% figure gives understanding that a true advocacy organization could use.
So how did they come to the idea that the autism prevalence increased by 20%? They skipped to page 13 and took one part of one paragraph out of context and, well, cherry picked. Completely unsurprising. They skipped over pages of data showing that we are failing to identify–and, therefore provide adequate services for–autistic minority children.
Sadly, AoA and their allies have spent over a decade denying this huge issue. The reason is obvious: it doesn’t fit into the “vaccines cause autism” narrative. So rather than push for better identification and better services for minorities, they’ve sacrificed these communities in for their political message.
It’s disgusting.
They didn’t dig any deeper into these numbers, even though the data were right in front of them. Also completely unsurprising. If they were the sort of people who dig into data and question, they wouldn’t be pushing the idea that vaccines cause autism. Seriously.
Here’s the section they are relying upon:
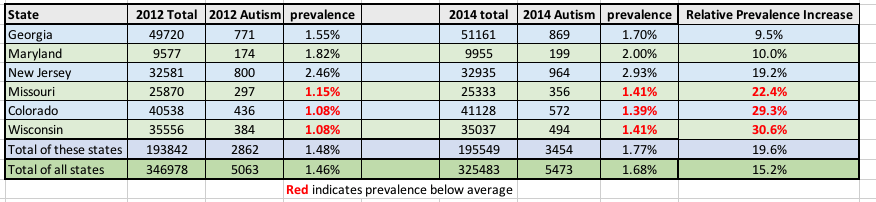
Among the six ADDM sites completing both the 2012 and 2014 studies for the same geographic area, all six showed higher ASD prevalence estimates for 2012 compared to 2014, with a nearly 10% higher prevalence in Georgia (p = 0.06) and Maryland (p = 0.35), 19% in New Jersey (p<0.01), 22% in Missouri (p = 0.01), 29% in Colorado (p<0.01), and 31% in Wisconsin (p<0.01). When combining data from these six sites, ASD prevalence estimates for 2014 were 20% higher for 2014 compared to 2012 (p<0.01).
So, if you only pick the states where there were data in both this study (called 2014 because that’s when the data were collected to be analyzed) and the previous (2012) study, you get about a 20% increase (click to enlarge).

But what happens if you ask “why?” As in, why do these states show a larger increase than the entire group?
I put some numbers in red and bolded them for emphasis. Those are states with lower than average autism prevalences. Take a moment to think about that–the states with low autism prevalences are showing larger prevalence increases than other states. Start with a low number, and you are bound to get bigger percentage increases.
Missouri, Colorado and Wisconsin started out with very low identification rates. They’ve improved their identification rates. What if someone were to ask, “how did they do that? Can we use that elsewhere to serve more unidentified autistic children?”
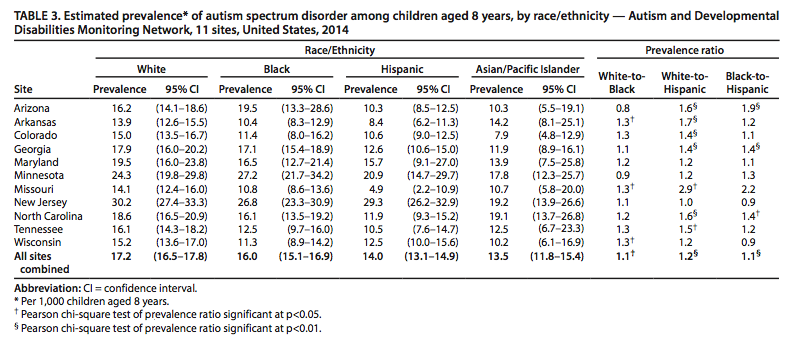
I’m sure the cherry-picking “let’s find a reason to fit this into the vaccines-cause-autism story” groups have already focused on New Jersey in the above figure. New Jersey stands out–their autism rate increased by about 19% and they have a much higher autism prevalence rate. New Jersey also stands out for another reason: they aren’t lagging in identifying black or Hispanic autistic children:
In New Jersey, there was almost no difference in ASD prevalence estimates among white, black, and Hispanic children. Estimates for Asian/Pacific Islander children ranged from 7.9 per 1,000 (Colorado) to 19.2 per 1,000 (New Jersey) with notably wide CIs.
Wouldn’t it be great if someone were to say, “how did New Jersey close the gap in identifying some minority groups?”
Groups advocating for a better future for disabled people would do that. People trying to keep the failed “it’s all vaccines fault” idea alive won’t.
Some people will be confused, and understandably so, at this point. These are “autism prevalence” numbers. Doesn’t that mean that this is a complete and accurate count of the number of autistic kids in each location? No, they aren’t. The people at the CDC are working hard and doing a good job with the information they have. But this is a review of existing records, not a test of each individual kid. The CDC have access to medical and/or school records (it varies by location what sort of records they have).
Keep in mind–the CDC autism prevalence numbers aren’t “these are the absolute accurate numbers for how many kids are autistic”. We are missing identifying kids. Doctors are missing autistic kids. Schools are missing autistic kids. The CDC tries to make up for this by reviewing the records to determine which kids are autistic (i.e. they don’t just count existing diagnoses in the records–they “diagnose” from the records). But they still miss kids in their counts. We need to get better. The fact that New Jersey isn’t leaving minority kids behind is huge. The fact that lagging states are catching up is huge.
Doing things right–checking on numbers is hard. It takes time. AoA not only doesn’t take the time to be careful (which is typical for the “vaccines cause autism” groups), they know that it’s the simple message that scares people. “Autism increased by 20%”!!!! It may only take 5 minutes to actually dig and see what’s going on. But that’s five minutes most people don’t have time for.
Which is the long winded way to say:
A lie can travel halfway around the world before the truth can get its boots on
Groups like AoA live and breathe on taking advantage of that. They were fake news long before the term was coined.
That said, I knew with the new autism prevalence numbers people would misuse them. It’s pretty obvious. They’ve used that misinformation to drag parents into a world of guilt and shame for being part of vaccine injuries that, in at least the vast majority of cases, didn’t happen. Even more, the autism-is-a-vaccine epidemic community had the resources for over a decade to make a real difference in the lives of autsitic people. As we watch autism fade a bit from the public’s view, it’s difficult to not cry a bit for the lost opportunity. It’s that, not their failed logic or twisted facts that is why I wrote the above.
—
By Matt Carey
Tags: Autism, prevalence




Recent Comments